INTRODUCTION
Sleep bruxism (SB), a stereotyped oromandibular activity during sleep, is characterized by teeth grinding and clenching [1]. SB was classified in the revised version of the 2005 International Classification of Sleep Disorders as a “sleep-related movement disorder” [2]. Based on bed-partner reports of tooth grinding, SB occurs in 5–8% of the adult population. The prevalence of SB decreases from childhood at 14–20% to old age at 3%. No gender difference in SB prevalence has been noted [3].
The evolution of definition and classification of SB has allowed this entity to become more distinct and homogenous. Increased focus facilitates research activities, resulting in improved understanding of etiological factors and physiological processes associated with SB. Despite many recognized risk factors for SB, its etiology and pathophysiology are yet to be established. There is convincing evidence that bruxism is part of an arousal response and sleep-related movement disorder. In short, bruxism is mainly mediated centrally, not peripherally [4]. SB is no longer considered to be simply related to mechanistic factors such as occlusal discrepancies or due to psychological issues such as stress, anxiety, depression, or a combination of them.
SB is considered as primarily a sleep-related movement disorder with a yet to be discerned multifactorial etiology and complex multisystem physiological processes [5]. SB has many clinical symptoms, including a tooth-grinding noise that might be reported by bed partner, pain in the temporomandibular joint and masticatory muscles, headache (especially in the temporal zone when the patient wakes up in the morning), tooth hypersensitivity, and morning jaw stiffness. Some clinical signs include abnormal tooth wear, tongue indentation, linea alba, hypertrophy of masseter muscles, and breakage of fillings and/or teeth. However, many of the deleterious effects of SB are permanent; clinically speaking, it is sometimes difficult to ascertain [6].
MANAGEMENT OF SLEEP BRUXISM
There are various treatment modalities for the management of SB, including occlusal appliances, behavioral approaches, and pharmacological management. However, none of them has been reported to be able to treat SB perfectly [2]. Treatment of bruxism is indicated when the disorder causes any of these aforementioned problems. Treatment is designed primarily to prevent further damage to the teeth. Unfortunately, there is no evidence that bruxism can be permanently altered by dental, behavioral, or pharmacological intervention. Clinician’s choice of management option is driven by the need to protect orofacial structures from damage and relieve any accompanying pain related to sensory complaints.
Occlusal Approaches
Oral appliances may reduce bruxism, muscular activities, and myofascial pains. Oral appliances can generally prevent tooth wear and injury and perhaps reduce night time clenching or grinding behavior rather than altering a causative malocclusion. Although these appliances can help reduce muscle pain, they are unlikely to significantly reduce nocturnal behavior. These appliances are worn every night by bruxers (Fig. 1) [7]. They can protect dental surfaces and relax masticatory muscles. They have been extensively used in clinical practice. However, their exact mechanisms of action are still under debate. No evidence supports their role in stopping SB.
Behavioral Approaches
Nocturnal alarms have been used to treat bruxism. Typically, these devices monitor masticatory electromyography (EMG) activity or sounds. When the activity exceeds a threshold for a given period of time, an alarm sounds and wakes the bruxer to terminate the grinding/clenching behaviors. Because sleep is disrupted, patients who use nocturnal alarms may report sleepiness and difficulty in concentrating if an alarm is being used. Discontinuation of the alarm may lead to “Rebound” in the level of grinding.
Pharmacologic Approaches
The etiopathophysiology of SB is still unclear. However, considerable evidence indicates that monoamine neurotransmitters, especially dopamine, may play a role in the development of this disorder. A previous controlled study of dopamine precursor L-dopa, and a recent case report involving dopamine D1/D2 receptor agonist pergolide have demonstrated the effective use of dopaminergic agents for treatment of SB [8]. This supports the currently unproven hypothesis that dopamine depletion causes this disorder [9]. However, inconsistent results have been reported for another D2 agonist, bromocriptine. Medications for the management of bruxism have been studied increasingly over the last few years, including BoNT, anticonvulsant drugs, and selective serotonin reuptake inhibitor. Unfortunately, there is only limited evidence showing efficacy of any of these drugs. Most studies are case reports. Thus, no definite conclusions can be drawn. Despite studies have provided evidence that the dopaminergic system plays a crucial role in SB, the mechanism of psychotropic drug-induced bruxism is still poorly understood. Psychotropic drugs can also modulate other neurotransmitters. This may cause different and sometimes opposite effects on either awake or SB [9].
The most recent advocated pharmacological approach to manage pathological effects of nocturnal and diurnal bruxism is by injecting muscles of mastication with BoNT. Recent research studies have shown that BoNT is effective for controlling involuntary orofacial movements and secondary bruxism in patients with movement disorders (e.g., cranial dystonia) [10–13]. However, most relevant studies are case reports. Very few systematic studies have provided high-quality data for the management of SB. Lee et al. [14] have studied the effect of BoNT on nocturnal bruxism using a portable EMG device and found that BoNT injection can reduce the number of nocturnal bruxism events for up to 12 weeks. However, these data were assessed by automatic detections based on EMG threshold. This method has difficulty in discriminating between SB and other oral motor activities based on portable EMG. Although many studies have evaluated SB patients and normal non-bruxers using polysomnography (PSG) [15,16], only one study has used PSG to study the effect of BoNT on SB [17].
It is known that masseter and temporalis muscles are muscles related to SB [17]. Many case studies have reported injections of the masseter muscle, while others have injected both masseter and temporal muscles [18–20]. Although many people might think that the temporal muscle plays a smaller role in SB, it is likely that temporal and masseter muscles are involved in SB equally.
Only one study has evaluated the effect of a single BoNT injection on SB using PSG [17]. Results of that study showed that BoNT injection to masseter and temporalis muscles did not change the occurrence of rhythmic masticatory muscle activity (RMMA) episodes or orofacial activities. However, the amplitude of EMG burst during RMMA episodes was significantly decreased for muscles that received BoNT injection. There were no significant differences in usual sleep variables such as sleep efficiency, arousal index, sleep stages, or awakenings per hour between baseline and follow-up recordings [17].
These findings confirmed that the effect of BoNT on jaw motor activity during sleep was characterized by a reduction in the intensity of contractions in injected muscles rather than by a reduction in event occurrence [21–24]. In that study, BoNT at a dose of 25 U was usually injected into each muscles using a 1-mL-syringe with a 29-gauge, 0.5-inch needle. BoNT was injected into two to three sites of each subject’s masseter and/or temporalis muscles. The method of injection into masseter muscle is the same as the injection for masseter muscle hypertrophy. In the temporalis muscle, the first site was the prominent part of the anterior temporalis muscle that was observed when the subject was asked to clench. It was parallel to the eyebrow. The other two sites were 10 mm and 20 mm posterior from the first site [17].
ANATOMICAL RECOMMENDATIONS FOR SAFE BOTULINUM TOXIN INJECTION INTO MASSETER AND TEMPORALIS MUSCLE
Masseter Muscle
The injection of the masseter muscle in SB patient use the same technique as that used for masseteric hypertrophy injection. Botulinum toxin injection sites (blue dots) are separated by 1 cm in the center of the middle third of the masseter muscle. These two injection points are used for most females and for males with a narrow cheek, with 25 U of botulinum toxin being injected (Fig. 2).
Temporalis Muscle
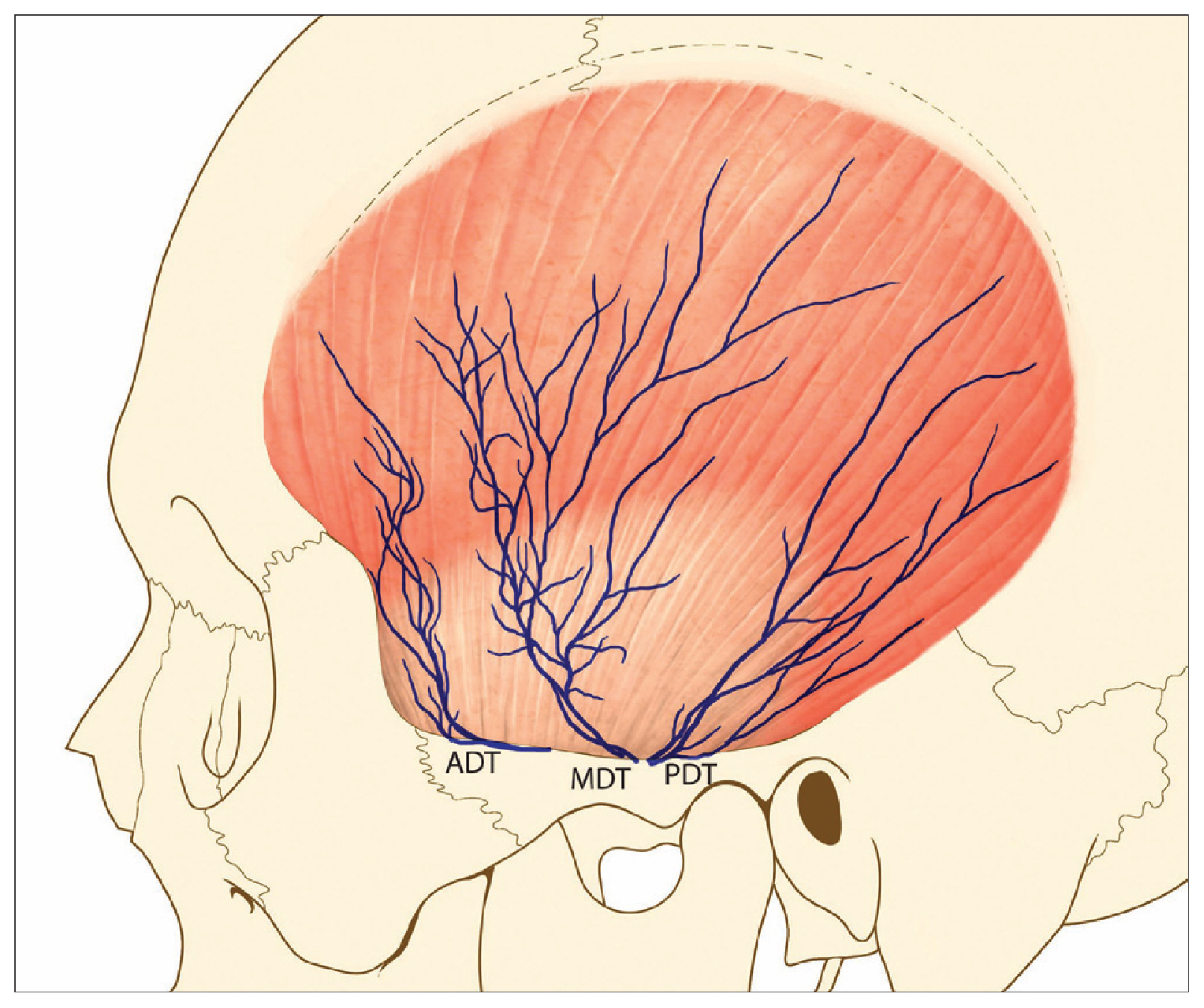
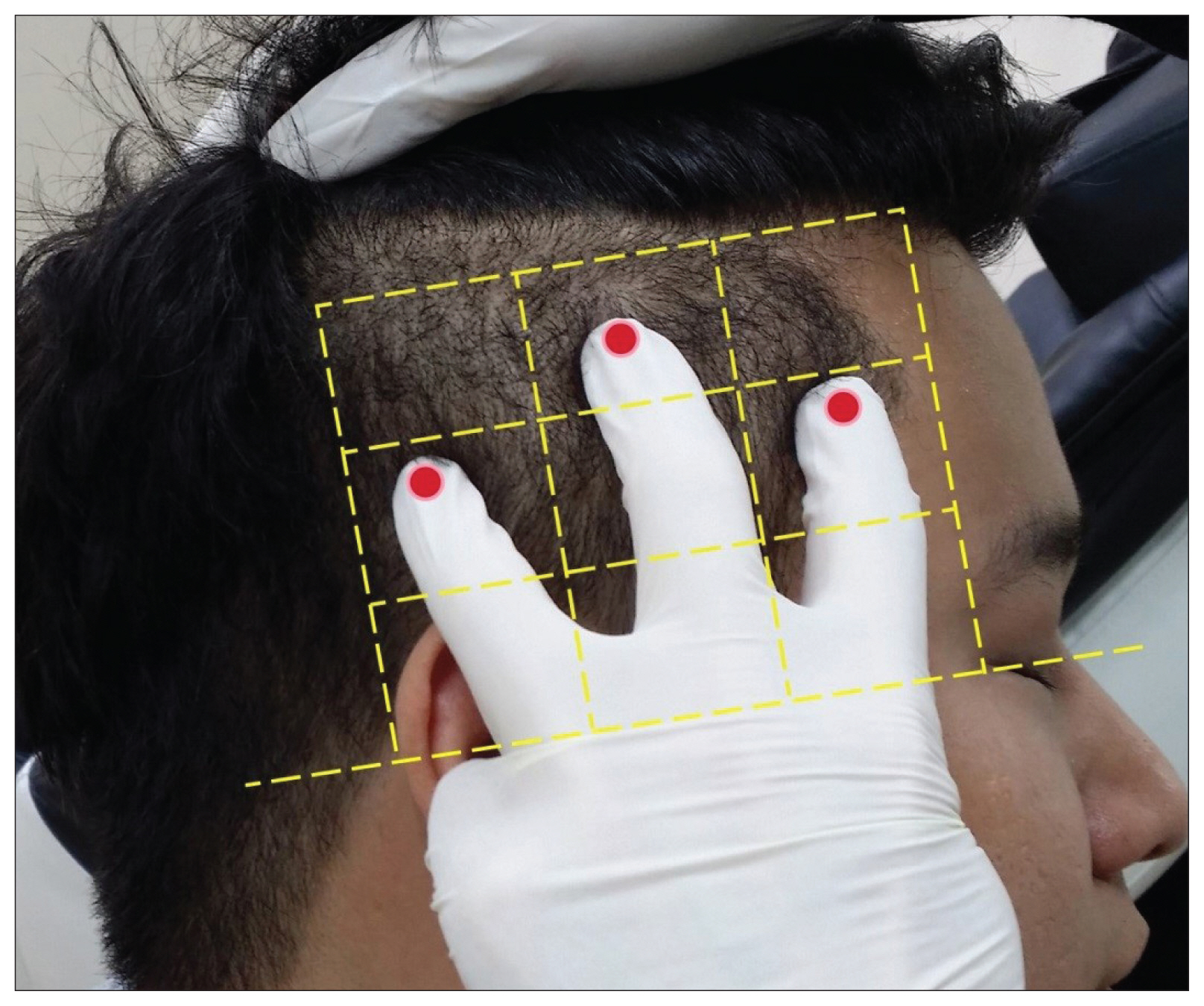
Lee et al. [25] have performed a study to simplify optimal temporal areas with a safe and reproducible approach for BoNT injections into the temporalis muscle. They carried out detailed dissections and measurements of structures in the temporal area to virtually represent a topographic mapping of postural relations among major anatomical structures, such as temporal branch of the facial nerve in the temporalis muscle of the temporal area (Figs. 3 and 4).
They proposed safe and reproducible injection sites in the form of compartments. It would be helpful to further specify the exact position of the injection site within the nine temporalis muscle compartments described herein, to enable clinician to perform injections with greater confidence.
CONCLUSION
SB and its consequences are complex. They require a committed personalized approach to change behaviors through oral appliances, behavioral approaches, and medications. The primary option for managing SB is still a full-arch oral appliance. For extreme cases, BoNT injections can be applied.