INTRODUCTION
Sleep helps to rehabilitate and restore both physical and mental health. It allows the body to control cellular growth and maintain hormone-focused metabolism [1]. The quantity of a person’s sleep can influence their behavior and health-related traits [2]. Age, sex, local residency, higher socioeconomic status leading to more than 24-hour entertainment at home with social networks or watching television, and lengthy working hours are associated with inadequate sleep [3,4]. However, it is still unclear how much sleep every individual needs. The amount of time required every 24 hours for best performance differs from person to person. A short sleep duration is defined as sleep lasting less than 6 or 7 hours on average over 24 hours. Long sleeping, on the other hand, is defined as sleeping for at least 9 hours [5]. Due to the adverse effects of irregular sleep patterns, the amount of sleep is likely to be associated with health-related outcomes, such as depression and anxiety. Notably, young individuals, such as students, are more likely to experience inadequate sleep, which can negatively affect learning, mood, and ordinary activities, leading to poor academic performance and healthcare costs [6]. Tapping more on niches, we can state that sleep deprivation has been shown to have an important effect on cognitive functions and motor activity. Especially, for medical students, these aspects are more important. This could be attributed to the demanding course contents and lengthy working hours. Healthcare students put in long hours at practice, hence are prone to inadequate sleep and its effects [7,8]. Ultimately, inadequate sleep might affect the community through accidents and medical errors [9]. This underlines the need for research on the effects of sleep quantity on students’ mental health. Therefore, the purpose of this study was to examine the relationship between sleep duration and depression and anxiety in first-year medical students at Neyshabur University of Medical Sciences (NUMS).
METHODS
Design and Study Population
A longitudinal survey for first-year medical students at NUMS was conducted. The survey collected information about students’ lifestyles and examined their relationship with academic success and health markers. The baseline data were collected in 2019 and 2020. For each year, data was collected during the enrollment period (late September to early October). The follow-up data were collected at the end of each academic year (annual follow-up). An informed consent, which involved informing the participants about their rights, the study’s goals, and the procedures used, was obtained from the participants [10]. All first-year students (n = 471) were asked to complete several questionnaires requesting demographic, socioeconomic, general health, and lifestyle data along with academic information.
The Declaration of Helsinki’s guiding principles were followed when conducting this study. The NUMS Ethics Committee gave their approval (Date: 05.10.2019/No: IR.NUMS. REC.1398.018).
Depression and Anxiety (Dependent Variables)
The research population’s level of depression was evaluated using the Persian version of the Beck Depression Inventory-II (BDI-II), which was validated in the Iranian population by Ghassemzadeh et al. [7]. Based on BDI-II, four categories (without depression, mild depression, moderate depression, and severe depression) are created. In this study, the categories of mild, moderate, and severe depression were compared to the category of no depression. The study population’s level of anxiety was assessed using the Persian version of the Beck Anxiety Inventory (BAI), which has been validated for the Iranian population by Kaviani and Mousavi [8]. Similar to the depression questionnaire, four groups (without anxiety, mild anxiety, moderate anxiety, and severe anxiety) were developed, and likewise, the categories of mild, moderate, and severe anxiety were compared to the category of no anxiety.
Sleep Duration (Independent Variable)
A question from the Pittsburgh Sleep Quality Index (PSOI) was used to measure the average number of hours that the students slept each night over 1 month. Three categories of sleep duration were established: inadequate (less than 7 hours), adequate (≥ 7 to < 9 hours), and excessive (equal to or more than 9 hours). Alimirzaei et al. [9] validated the Persian version of the PSOI in the students of Kerman University of Medical Sciences (a province in southeast Iran).
Covariates
In this study, factors such as sex (female vs. male), age (≤ 20 years old vs. > 20 years old), marital status (single vs. married), family residency (urban vs. rural), family size (≤ 4 vs. > 4), ethnicity (Fars vs. other), smoking (no vs. yes), body mass index (BMI) (< 25 vs. ≥ 25 kg/m2), physical activity (low vs. moderate vs. high), and family wealth index (WI) (poorest vs. poor vs. moderate vs. rich vs. richest) were included as covariates. In this study, WI evaluated the family’s economic situation, and it was calculated using principal component analysis based on the student’s family’s ownership of some assets.
Statistical Analysis
The variables’ frequencies, percentages, means, and standard deviations (SDs) were calculated using the descriptive analysis. At the univariate level, the association between the study population’s characteristics and different levels of dependent variables (depression and anxiety) was evaluated using the chi-square test. The independent associations of sleep duration with depression and anxiety were assessed using multinomial logistic regression models. The significance level was set at p < 0.05, and Stata 14 (StataCorp LLC., College Station, TX, USA) was used for all statistical analyses
RESULTS
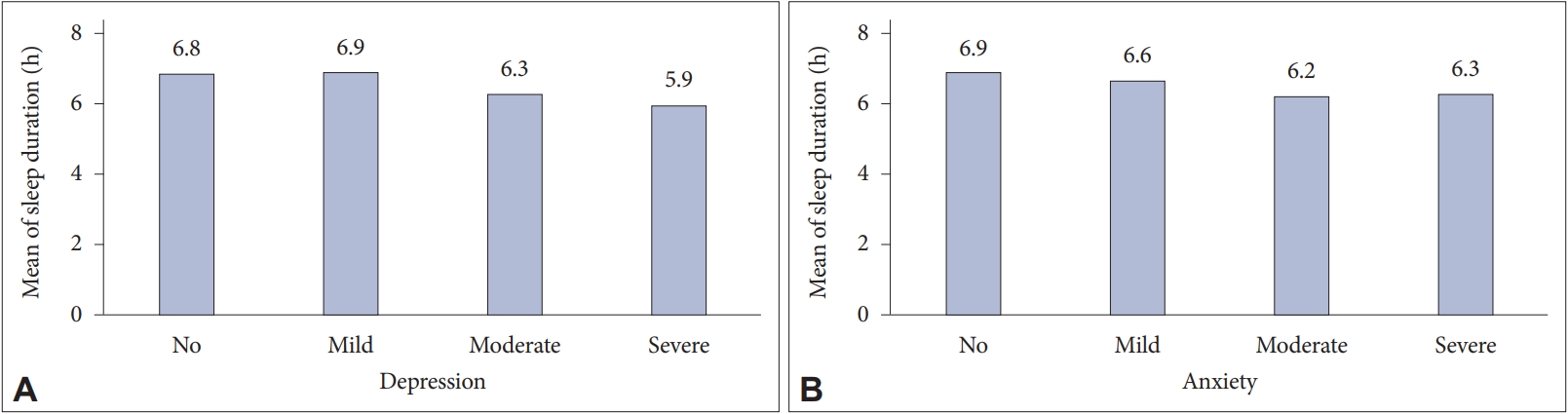
The mean age of the students who participated in the study was approximately 22 years, and most of them were female (62.4%). More than 78% of the participants lived in urban areas, and less than 16% of them were married. Table 1 lists other characteristics of the study participants. The prevalence of inadequate and excessive sleep duration was 41.8% and 6.4% of the students, respectively, while approximately 52% of the students reported adequate sleep duration. As shown in Table 1, more than 20% of the students reported depression (mild = 10.2%, moderate = 7.0%, and severe = 4.2%). Also, approximately one-third of the students reported anxiety (mild = 20.6%, moderate = 7.9%, and severe = 3.4%) (Table 1). Fig. 1 presents the mean sleep duration based on different levels of depression and anxiety. As shown in Fig. 1A, the mean sleep duration in students with moderate and severe depression was lower than in students with no depression. Also, the mean sleep duration in students with mild, moderate, and severe anxiety is lower than in students with no anxiety (Fig. 1B).
Association of Sleep Duration and Depression
The results of the unadjusted and adjusted associations between sleep duration and depression are shown in Tables 1 and 2, respectively. Significant associations were observed between sleep duration and depression in the unadjusted (p = 0.005) and some of the adjusted (p < 0.05) models (Table 2). As shown in Table 2, in the adjusted models, comparison results of the inadequate sleep category with the adequate sleep category showed a significant association with moderate and severe depression. In this setting, after adjusting for all covariates (model 3), we observed that the odds of moderate and severe depression in individuals with inadequate sleep were three times higher compared to individuals with adequate sleep. In individuals with mild depression, there was no significant association observed between sleep duration and depression in all the adjusted models (p > 0.05). There was no association observed between excess sleep duration and depression in all the adjusted models (p > 0.05).
Association of Sleep Duration and Anxiety
The association between sleep duration and anxiety is shown in Tables 1 and 3. The sleep duration was not significantly associated with anxiety in the unadjusted (p = 0.053) (Table 1) and most of the adjusted (p > 0.05) models (Table 3). As presented in Table 3, in the adjusted models, comparison results of the inadequate sleep category with the adequate sleep category showed a significant association with moderate anxiety in the study population. In this regard, when the models were adjusted for studied covariates, we observed that the odds of moderate anxiety in individuals with inadequate sleep was three times higher than in individuals with adequate sleep. In individuals with mild and severe anxiety, there was no significant association observed between sleep duration and anxiety in all the adjusted models (p > 0.05). Moreover, there was no association observed between excess sleep duration and anxiety in all the adjusted models (p > 0.05).
DISCUSSION
Sleep takes approximately one-third of our lives and hence is an integral aspect of life. Adequate sleep is essential for physical and mental development and stability. Therefore, inadequate sleep not only devitalizes physical and mental functions, and leads to weaker work productivity, but may also cause mental disorders like depression and anxiety [11]. Consequently, inadequate sleep can have deleterious effects on society and individuals.
According to our results, more than 40% of the students in this study had inadequate sleep duration. Similarly, in a study conducted at King Abdulaziz University, Ibrahim et al. [12] found that the students who enrolled in the basic educational years suffered higher rates of inadequate sleep compared to the comparative groups. Also, findings from an investigation on medical students in Egypt in 2017 indicated that students in their first years (preclinical years) reported higher scores of inadequate and poor sleep compared to the counter groups [13]. Looking at the binary pole of findings, the present study is inconsistent with some findings [14,15]. For instance, Yazdi et al. [16] showed that senior students suffered higher levels of inadequate sleep. Also, Frank et al. [17] observed that the mean night sleep duration in freshman students was more than in the other students.
Using multinomial logistic regression models and after adjusting for studied covariates, the results of this study showed that the odds of moderate and severe depression in individuals with inadequate sleep were three times higher than in individuals with adequate sleep. Depression is considered the greatest contributor to global disability and accounted for 5% of disability rates in 2016 [18]. Previous studies have shown that depression is associated with genetics, behavioral, physical, and socioeconomic factors [19,20]; in line with these contributing factors, duration and pattern of sleep have been found to be risk factors for depression [21,22].
Inadequate sleep among healthcare students has been documented and with trivial differences in the results, the current study is a corroborating trace for the previous findings [23,24]. Previous literature has reported that inadequate sleep is tied with depressive and anxiety symptoms. Johnson et al. [25] propounded that sleep duration is a robust predictor of successive affective disorders. At one-year follow-ups in university, it was asserted that abatement in sleep duration potentially leads to a reduction of depression incidence [26]. Consistent with our study findings, Choi et al. [27] found that inadequate sleep was associated with depression; that is, individuals with severe depressive disorders suffer short sleep duration and low sleep efficiency. To further support our finding, stretches of evidence advocate that sleep problems mostly occur prior to depressive and anxiety symptoms and hence might be threatening bells for subsequent mental problems. Therefore, prompt and convenient interventions for sleep problems might deter the ensuing onset or aggravation of anxiety and depressive symptoms [28].
In the second part of multinomial logistic regression models, the analysis revealed that the odds of moderate anxiety in individuals with inadequate sleep were three times higher than in individuals with adequate sleep. In this study, in individuals with mild and severe anxiety, there was no significant association between sleep duration and anxiety in all the adjusted models. Inadequate and poor sleep has been one of the persistent predictors of enhanced anxiety levels in college students [29]. The relationship between sleep duration and anxiety in the current study is consistent with the previous literature. For instance, the results of two previous studies showed that inadequate sleep exacerbates the severity of anxiety symptoms and hence concluded that inadequate sleep and anxiety might facilitate probing treatment strategies [30,31]. The high reported value in moderate anxiety and inadequate sleep can be justified by the association between mental health and sleep quality. While the results of this study showed that sleeping for less than 7 hours increases anxiety severity by up to 14%, this finding is not statistically significant; therefore, we cannot rely on it. As shown in Table 1, the number of individuals in this range was small (n = 16); thus, generalizing these results should be done with care.
Strengths and Limitations
Despite the contributions of the study, it has several shortcomings. First, since this is a cross-sectional study, we are unable to conclude the causes. Second, we recruited students from only one university and there was a potential for recall bias from the study population; therefore, the findings might not be generalizable to all non-healthcare students’ samples. Third, additional confounding factors may have impacted the study’s data. Therefore, it is necessary to conduct a study with a larger sample size that takes into consideration other variables as well. Fourth, the self-reported instrument was employed to capture sleep duration, which could in turn cause bias. Lastly, the current study failed to take into account a clinical diagnosis of anxiety and depression. Despite these limitations, this study has several advantages. First, the effect of numerous confounding factors was controlled when we used multinomial logistic regression models to analyze the association between sleep duration with depression and anxiety in this study. Second, recruiting a sample of students at NUMS that is typical of both clinical and nonclinical medical students, is considered another edge. Last, although the current study recruited a sufficient sample size, the researchers had their centralization only on specific groups of students (freshmen students).
Conclusions
The findings of this study confirmed that sleep duration is significantly associated with depression and anxiety among freshmen students at NUMS. Therefore, evaluating sleep duration and its association with depression and anxiety in medical students might lend a hand in the early diagnosis and management of mental health. Therefore, to improve medical students’ sleep problems and consequently prevent depression and anxiety, it is essential for the concerned officials to develop and implement interventional programs.