INTRODUCTION
Coronavirus disease 2019 (COVID-19) is an infectious disease that is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). This new type of coronavirus was first detected in the Chinese city of Wuhan in late 2019. So far, the virus has spread to many countries worldwide. On March 11, 2020, the World Health Organization (WHO) declared COVID-19 a pandemic, due to its high prevalence and infection rate [1]. Globally, as of July 11, 2022, there were 552504629 confirmed cases of COVID-19, including 6347816 deaths reported to the WHO. At the same time, based on the COVID-19 data Task Force in Indonesia, there were 6112986 confirmed cases, 20343 active cases, 5935845 (97.1 %) recovered cases, and 156798 (2.6%) deaths [2]. The COVID-19 pandemic has resulted in the government implementing policies restricting activities, such as lockdowns, large-scale social restrictions, social confinement, staying at home, and the restriction of outdoor activities, to reduce the transmission of this virus. These restrictions have had a profound impact on the unprecedented change in human life and also caused the general public to suffer from stress, depression, anxiety, feeling sick, panic, and being unable to stop thinking about COVID-19, which contribute to insomnia [3-5].
Insomnia is characterized by difficulty in falling asleep and maintaining sleep, resulting in impaired daytime functioning. According to the American Academy of Sleep Medicine, insomnia can be diagnosed if sleep difficulties are present for 3 nights per week and last for longer than 3 months [6]. The prevalence of insomnia ranges 10% to 15% in the general population [7]. In Indonesia, the prevalence of insomnia is about 10%–11% [8,9]. Sleep disorders can also be caused by work pressures, financial problems, obligations to family, and social relationships, as well as health problems. The social impact of insomnia can decrease the quality of life, increase work absences, diminish productivity, cause traffic injuries, and impair physical health [10-13]. Many studies link the incidence of insomnia with several health problems, such as type 2 diabetes, hypertension, cancer, cardiovascular disease, and heart failure [14-17].
Since the first wave of the COVID-19 pandemic, new cases of insomnia have emerged in various countries worldwide and have increased the prevalence of insomnia [18-20]. This is because the restrictions on activities lead to more time to take a nap or snack, or play on smartphones in bed, which can reduce sun exposure and affect circadian rhythms [21,22]. A study proved that spending more than 1 hour in bed during stay-at-home and not going to work are two of the reasons most young women living in the epicenter area and at high risk of COVID-19 suffer from insomnia [21]. Stress has become one of the most common mental health problems during the COVID-19 pandemic, which has also exacerbated the symptoms of chronic insomnia patients, such as poorer sleep quality, longer sleep latency, shorter sleep duration, sleep disturbances, lack of sleep efficiency, and impaired daytime function [23,24].
An international collaborative study revealed that symptomatic rates of insomnia (36.7%) and insomnia disorder (17.4%) were approximately twofold higher during the first wave of a pandemic, because prevalence rates are typically reported in non-pandemic times of COVID-19 [18]. A study in Greece found that as many as 37.6% of a sample of 2472 people reported insomnia during the COVID-19 epidemic, particularly women and urban residents [25]. A study conducted in Milan, Italy with 400 participants, including 307 students and 93 workers, found that the prevalence of insomnia before the COVID-19 pandemic was 24% and, during the COVID-19 pandemic, increased to 40%. Additionally, workers with difficulty falling asleep increased from 15% to 42%. Lockdowns during the COVID-19 pandemic affected students more than workers and women more than men [19].
The COVID-19 pandemic is strongly associated with the prevalence of sleeplessness. Insomnia was experienced by 24.66% of the 1172 respondents diagnosed with psychotic disorders as a result of the COVID-19 pandemic, according to a study [26]. Additionally, the COVID-19 pandemic has aggravated the symptoms of people diagnosed with sleeplessness. In a study by Yang et al. [23], assessing the sleep status of 738 patients with a diagnosis of chronic insomnia using the Pittsburgh Sleep Quality Index (PSQI) yielded an average score of 11.28, significantly higher than the maximum score after 8 weeks of follow-up, indicating a statistically significant difference in poor sleep quality during the COVID-19 pandemic.
The map of the spread of COVID-19 in Indonesia establishes that Central Java Province is ranked third highest in the distribution of COVID-19 cases as of July 11, 2022, with a percentage of 10.3% [27]. Indonesia has imposed restrictions on community activities, and this regulation carries with it a high risk of psychological disorders, which, as has been proven in previous studies, can be one of the causes of insomnia. This study aims to describe insomnia prevalence before and during the COVID-19 pandemic in Indonesia.
METHODS
Study Design
This cross-sectional survey was conducted on the general population in the city of Surakarta, Indonesia. The survey was conducted in two stages; the first-stage data was taken to ascertain the prevalence of insomnia in general, and was carried out from October 2019 to January 2020. The second survey to determine the prevalence of insomnia during the COVID-19 pandemic was carried out from February 2020 to May 2020. This study was carried out in five sub-districts areas in Surakarta city: Banjarsari, Jebres, Serengan, Laweyan, and Pasar Kliwon.
Participants
The study participants consisted of two groups. The participants before the COVID-19 pandemic amounted to 456 subjects, while the participants during the COVID-19 pandemic amounted to 1254 subjects. Participants were selected using the purposive sampling method. All participants were selected based on the following criteria: living in Surakarta city, aged 15–44 years (productive age), and experiencing sleep problems.
Ethical Approval and Consent of Participants
This study was conducted in accordance with the principles of the Declaration of Helsinki. The Research Ethics Committee of the National University of Malaysia approved the study protocol (Date: 19 March 2020/Approval No: UKM.FSK.800-2/27/9 (NN-2020-036). Each participant consented to participate in the study by confirming informed consent after being informed of the purpose of the study.
Assessment
The Insomnia Severity Index (ISI) is designed to measure insomnia severity. This research uses an ISI Indonesian version, the ISI–INA. The ISI–INA contains 7 items: difficulty falling asleep, difficulty staying asleep, waking up too early, dissatisfaction with sleep patterns, interference of sleep difficulties with daytime functioning, noticeability of sleep difficulty by others, and distress-caused sleep difficulties. The ISI–INA has high validity and reliability for detecting insomnia cases with r values of 0.988 for item 1, 1.00 for item 2, 0.993 for item 3, 0.971 for item 4, 0.989 for item 5, 0.983 for item 6, and 0.991 for item 7, and Cronbach α of the first and second examinations being 0.989 and 0.929, respectively [28]. Participants filled out the ISI–INA questionnaire according to their sleep experience over the previous one month. Scoring items used a 5-point Likert scale (0–4), generating a score ranging from 0 to 28. We identified which participants met the criteria by using cut-off scores of ≥ 8 for subthreshold insomnia, and a cut-off of ≥ 15 for moderate-to-severe insomnia [29]. The higher total ISI score meant the more severe suffering of the participant from clinical insomnia.
Statistical Analysis
The data analysis was conducted using SPSS Statistics for Windows (Ver 25; IBM Corp., Armonk, NY, USA). Quantitative data included the participant characteristics of age, residence, educational history, employment, severity of insomnia, and mean score of 7 items of the ISI–INA, which were analyzed by descriptive test and are presented in the table of distribution frequency and percentage (%). This research grouped participants into 4 groups based on the total ISI–INA scores they obtained. The four groups were those with no clinically significant insomnia (0–7), subthreshold insomnia (8–14), moderate insomnia (15–21), or severe insomnia (22–28) [30].
RESULT
Characteristic Sample
This study’s participants were 1710 people, consisting of 456 participants before the pandemic and 1254 participants during the pandemic. Table 1 shows the participant characteristics, including age and residence.
A total of 1710 participants were all in the productive age range. Of the 456 participants before the COVID-19 pandemic, the average age was 21.63 ± 5.01 years, and most were 20 years old (44.7%); while of the 1254 participants during the COVID-19 pandemic, the average age was 21.63 ± 1.96 years, and most were 22 years old (21.5%). Data on where participants live were used to see the distribution of insomnia cases before the pandemic and after the pandemic. The 1710 participants in this study covered the districts of Banjarsari, Jebres, Serengan, Laweyan, and Pasar Kliwon. Of the 456 participants before the COVID-19 pandemic, the majority lived in the Jebres district (37.1%), and of the 1254 participants during the COVID-19 pandemic, the majority lived in the Laweyan district (22.4%).
Severity of Insomnia
Table 2 summarizes the analysis of the total ISI score and severity of insomnia before and during COVID-19. The mean total ISI–INA score before COVID-19 was 13.83 ± 4.47, while during COVID-19 was 12.54 ± 5.49. According to the categorization of insomnia by total ISI–INA scores, the average total score before and during COVID-19 was at the subthreshold level of insomnia (8–14). The survey results found that most participants before and during COVID-19 have experienced subthreshold insomnia at 45.6% and 42.1%, and moderate insomnia at 41.2% and 35%, respectively. Only 5.0% of participants before COVID-19 and 3.2% of participants during COVID-19 suffered from severe insomnia. The results show that the prevalence of insomnia during the COVID-19 pandemic has decreased, compared to before the COVID-19 pandemic. Analysis of differences between before and during the COVID-19 pandemic in total score and the level of insomnia severity both obtained a p-value of < 0.001.
The Effect of Education and Employment on Total ISI–INA Scores During COVID-19
Table 3 summarizes the analysis of the effect of education and employment on total ISI–INA scores during COVID-19. The most recent education of most participants during COVID-19 was senior high school (69.2%) and the employment of most participants was college students (65.9%). The results of the analysis found the effect of last education (0.002) and employment (0.001) on the total ISI–INA score, which was used as an indicator of insomnia.
Seven Items of ISI–INA
Table 4 summarizes the analysis of the mean score on the 7 items of ISI–INA before and during COVID-19. Participants before COVID-19 responded to questions regarding the difficulty of falling asleep with an average of “moderate” responses (2.12 ± 0.85), difficulty staying asleep with an average of “moderate” responses (1.58 ± 0.99), problems waking up too early with an average of “mild” responses (1.38 ± 0.99), dissatisfaction with sleep with an average of “dissatisfied” responses (2.58 ± 0.87), interference of sleep difficulties with daily activities with an average of “somewhat interfere” responses (2.31 ± 1.04), noticeability of sleep problems by others with an average of “somewhat noticeable” responses (1.87 ± 1.01), and worry about difficulty sleeping with an average of “somewhat worried” responses (1.99 ± 1.06).
Participants during COVID-19 responded to questions regarding the difficulty of falling asleep with an average of “moderate” responses (1.50 ± 1.09), difficulty staying asleep with an average of “mild” responses (1.20 ± 1.01), problems waking up too early with an average of “mild” responses (1.17 ± 0.96), dissatisfaction with sleep with an average of “neutral” responses (2.23 ± 1.12), interference of sleep difficulties with daily activities with an average of “somewhat interfere” responses (2.43 ± 1.18), noticeability of sleep problems by others with an average of “somewhat visible” responses (2.04 ± 1.15), and worry about difficulty sleeping with an average of “somewhat worried” responses (1.99 ± 1.19).
Analysis of differences between before and during the COVID-19 pandemic on items of difficulty falling asleep, difficulty staying asleep, waking up too early, and dissatisfaction with sleep patterns obtained a p-value of < 0.001. The p-value on the item of noticeability of sleep problems by others was 0.009, on the item of interference of sleep problems on daily activities was 0.014, and on the item of worry about difficulty sleeping was 0.963.
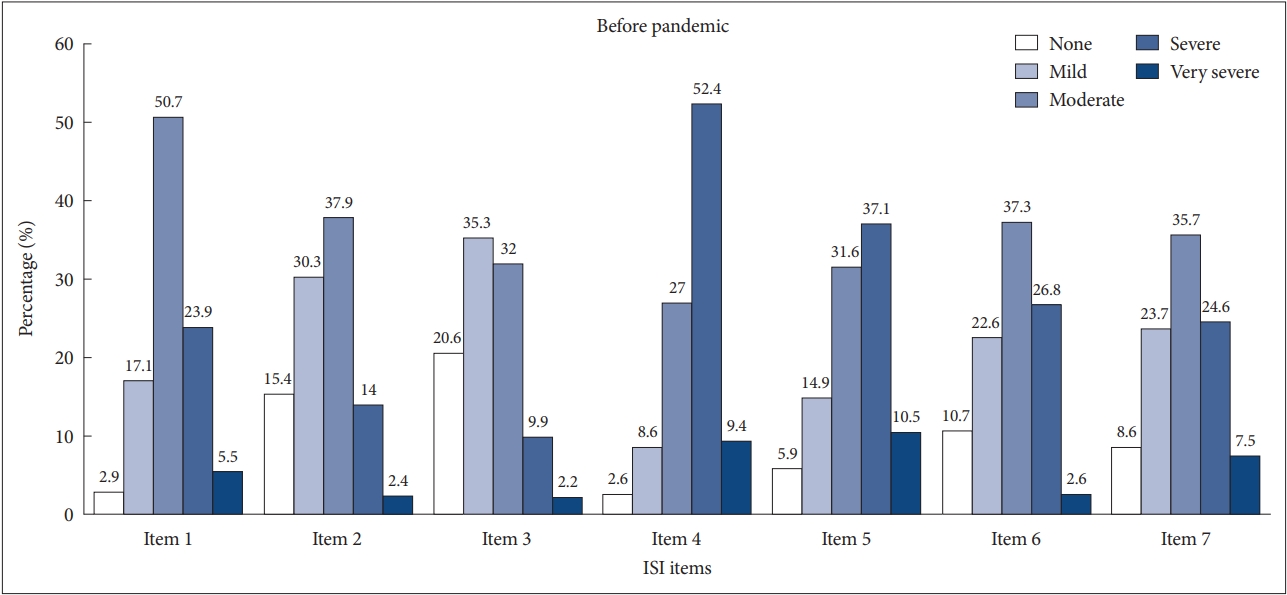
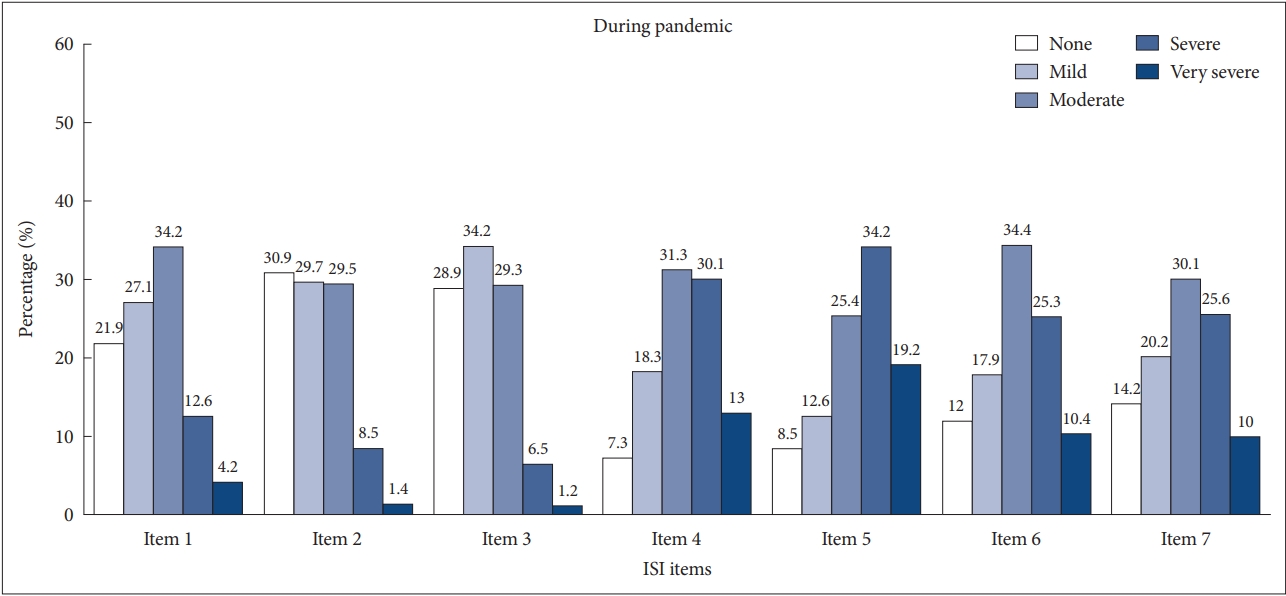
Fig. 1 shows each option selected by the participant for all 7 ISI items before the pandemic, and Fig. 2 during the pandemic. Based on both Figs. 1 and 2, the difference in the average of the most responses is seen in item 2 (difficulty staying asleep) and item 4 (sleep dissatisfaction). The average on most responses in both items 2 and 4 has decreased in severity during COVID-19. Fig. 1 shows that the most responses about the difficulty of staying asleep were “moderate,” and in Fig. 2, the most responses were “none.” Fig. 1 shows that the most responses about sleep dissatisfaction were “severe,” and in Fig. 2, the most responses were “moderate.”
DISCUSSION
This study aimed to use a cross-sectional survey to explain the prevalence of insomnia events before and during the COVID-19 pandemic. This study’s participants were 1710 people consisting of 456 participants before the pandemic and 1254 participants during the pandemic. A total of 1710 participants were all in the productive age range. The average age of participants before COVID-19 was 21.63 ± 5.01 years, and most of the participants were 20 years old (44.7%), while during COVID-19, the average age of participants was 21.63 ± 1.96 years, and most of the participants were 22 years old (21.5%). The 1710 participants in this study covered the districts of Banjarsari, Jebres, Serengan, Laweyan, and Pasar Kliwon. Before the COVID-19 pandemic, most of the participants lived in the Jebres district (37.1%), while during the COVID-19 pandemic, most of participants lived in the Laweyan district (22.4%).
Based on the results of the Mann–Whitney’s analysis, there was a difference in the total score of ISI–INA and level of insomnia before and during the pandemic (p < 0.05). Based on the percentage of insomnia rates, insomnia cases tended to decrease during the COVID-19 pandemic. The prevalence of subthreshold insomnia (≥ 8) both before and during the pandemic was 45.6% and 42.1%, moderate insomnia (≥ 15) was 41.2% and 35%, and severe insomnia (≥ 22) was 5% and 3.5%, respectively. Although the insomnia prevalence rate shows a decrease, the prevalence of insomnia in this study is still relatively high, compared to the international prevalence of insomnia before the pandemic of 10%–15% and during the pandemic of 20%–35% in the general population [7,18]. The prevalence of insomnia was stated to also be still quite high because the inclusion criteria of participants in this study were those who experienced sleep disorder problems. The high prevalence of insomnia in this study was greater than in the study by Voitsidis et al. [25] in 2020 of the Greek population during the pandemic, which research results obtained the prevalence of insomnia disorders of 37.6%. This percentage is greater than the worldwide prevalence of insomnia, indicating worsening sleep disorders during the COVID-19 pandemic.
The result of Mann–Whitney’s analysis shows that there was a significant difference in all ISI items (p < 0.05), except for the item of worrying caused by sleep difficulty (p ≥ 0.05) (Table 4). This difference can be caused by the number of participants taking the survey during COVID-19 being very much more than that before COVID-19; this difference causes the percentage of each response on each item to be different, and mostly reduced. The highest percentage of responses on items 2 (difficulty maintaining sleep) and 4 (dissatisfaction with sleep patterns) also differed before and during COVID-19.
The percentage of severity staying asleep has decreased during the pandemic (Figs. 1 and 2); this may be because many participants have no obstacles, such as work and other activities, when going to bed, so feel calm about falling asleep. Unfinished work and other activities that we want to do when we are about to fall asleep usually disturb the tranquility in our sleep, making it difficult to maintain sleep, and resulting in waking up too early. Sleep satisfaction increased during the pandemic, along with reduced difficulty falling asleep, maintaining sleep, and waking up too early that most participants experienced during the pandemic. The percentage of the interference of sleep difficulties with daily activities and noticeability of sleep difficulties by others decreased during the pandemic, because most participants had mild sleep difficulties. On the other hand, there was no difference in the item of worrying about difficulty sleeping. The average choice for the response of the item both before and during COVID-19 was also the same at “1.99” or “somewhat worried” (Table 4). The situation before and during the pandemic did not affect participants’ concerns about sleep problems, because both before and during the pandemic, in general, difficulty sleeping does make a person worry.
This study’s finding is similar to the results of a systematic review that estimated the prevalence of insomnia from five studies in healthcare workers to be 38.9%. Insomnia prevalence differs by sex and occupation, with women and medical staff showing higher prevalence. Medical staff experienced higher levels of insomnia during the COVID-19 pandemic [31]. They faced many cases of COVID-19 and had little time to engage in positive activities to deal with stress. This study also found the effect of education history and employment on total ISI scores (insomnia indicator) during the pandemic. Most of the participants during COVID-19 had an education history that was senior high school (69.2%), and most of the participants were college students (65.9%). During COVID-19, all jobs can still be done online casually. So maybe they could still engage in positive activities to reduce the risk of stress during the COVID-19 pandemic and reduce the risk of insomnia. In this study, most participants were 22 years old (adolescent group), so it is possible that during the COVID-19 pandemic, even though they experience insomnia, they can still reduce it by engaging in physical activity to reduce stress.
This study’s results contrast with various studies, one of which is an international collaborative study that showed that the rates of insomnia symptoms (36.7%) and insomnia disorders (17.4%) increased to be about two times higher during the first wave of the pandemic than the prevalence rates previously reported, as usually reported in times of non-pandemic COVID-19 [18]. Marelli et al. [19] conducted a survey in Italy before and during the COVID-19 outbreak, which found an increase in bedtime hours, sleep latency, wake-up time, as well as worsening sleep quality and insomnia symptoms. In China, Li et al. [32] also found a 33.7% increase in the prevalence of sleep disorders during the pandemic. They suggested that insomnia may be associated with financial stress, social distance restrictions, travel restrictions, changes in daily life, mental illness, and the gender of women. Severe psychological stress (i.e., depression and anxiety) or having previous mental disorders increased the risk of insomnia symptoms during the COVID-19 pandemic [33]. There was no information in this study of the respondents having previous mental disorders. So they might have been able to engage in positive activities to reduce symptoms of stress and depression, and so not have insomnia [34].
Restrictions around staying at home have disrupted daily activities, such as waking up in the morning, showing up at work, and maintaining social and leisure activities that typically serve as a timeframe for sleep–wake rhythms to stay in tune with the day–night cycle [18]. A study by Cellini et al. [35] showed that during the lockdowns in Italy and Belgium, bedtime was significantly delayed, time spent in bed increased, and sleep quality was severely impaired. Their research during lockdowns in Italy and Belgium showed bedtime was delayed, because during the lockdown, participants tended to go to bed late and also get up in the morning later than usual, which caused sleep and wake rhythms to change greatly, and the time spent in bed to increase. Longer bedtimes not accompanied by an increase in sleep duration indicate less sleep efficiency. Decreased sleep efficiency is one of the factors causing poor sleep quality. Work–life imbalances, such as isolation environments, stress, anxiety, worry of being infected with the virus, and extreme uncertainty regarding the effective control of the disease from the COVID-19 outbreak, are risk factors that have worsened sleep in many health-care workers [36]. The study also revealed some interesting aspects related to sleep health. Health, financial implications, changes in social life, and concerns about daily life increased stress levels during the outbreak of the virus. Reduced fatigue and exposure to sunlight and increasing usage of electronic devices can also affect sleep homeostasis [25].
The decrease in the prevalence of insomnia in Surakarta can occur because surveys during COVID-19 occurred in the first wave of COVID-19. Many people are unaware of and do not believe in the existence of COVID-19 in the environment. People tend not to care about the existence of COVID-19 in Indonesia, because people do not take the COVID-19 pandemic seriously and excessively. It is likely that they also think COVID-19 is not easily spread or causes serious illness. So COVID-19 has not been something they are worried about. Over time, the spread of information about COVID-19 has made people better informed on the impact of COVID-19 on their mental health, sleep patterns, and quality of life. Therefore, many people have started engaging in positive activities, such as physical exercise and maintaining a healthy diet, which factors can relieve the symptoms of their psychological distress and sleep disorders [37]. Exercise is useful for improving the sleep quality and quality of life of insomniacs [38]. Individuals can also engage in diversionary activities to distract from observing COVID-19-related news to avoid potentially incorrect information. Good and correct knowledge of COVID-19 can also reduce anxiety [39]. Positive diversion activities, such as listening to songs, watching movies, painting, gardening, and cooking, can also be done during the stay-at-home order [5]. Such positive activities are effective in relieving and preventing symptoms of stress and depression [34,37]. The mass changes that have occurred and are felt by many people make them not feel alone in the face of this virus, and the high social support in the community also decreases psychological distress [40].
There are several strengths to this study. First, the symptoms of insomnia were assessed before and during the outbreak of COVID-19. Second, the Indonesian version of the ISI had high validity and reliability values. Third, this study has a relatively large sample. However, when interpreting the results, some limitations need to be recognized and considered. First, although data collection through online questionnaires did result in a large number of samples being obtained, researchers could not interview participants directly to find out more in-depth information about the insomnia experienced by participants. Second, most of the participants were young adults, because the online data collection process was only accessible to young adults, so the results of this study were less representative of the incidence of insomnia in older adults. In addition, the data on factors affecting insomnia is limited, so in its analysis, the decrease in the prevalence of insomnia is less profound. Thirdly, the total number of the subjects before COVID-19 pandemic was substantially less than the total number of the subjects during the pandemic, which could have resulted in the decrease in prevalence during the pandemic due to the wider distribution of participants.
In conclusion, the prevalence of insomnia in Surakarta studied during the COVID-19 pandemic is lower than before the COVID-19 pandemic. Overall, the incidence of insomnia in the Surakarta area both before and during the COVID-19 pandemic was still relatively high, so psychological and medical interventions were needed to overcome insomnia experienced. Therefore, it is necessary to explore the causes of insomnia and need specific interventions according to the cause of insomnia.