Foot Ulcers and Sleep Quality in Type 2 Diabetes Mellitus
Article information

Abstract
Background and Objective
The study aimed to investigate the sleep quality of type 2 diabetic patients with and without foot ulcers, to determine whether there was a difference in sleep quality between them, and to examine the effect of diabetic foot ulcers on sleep quality.
Methods
Our prospective cross-sectional study was conducted between April and September 2021 at the Family Medicine Diabetes Clinic and Diabetic Foot Clinic of the hospital. A total of 146 patients were included in the study, of whom 64 had foot ulcers and 82 did not, and met the inclusion criteria. The patients were administered a patient information questionnaire that included sociodemographic data, waist circumference, HbA1c, diabetes duration, diabetes complication information, as well as the Pittsburgh Sleep Quality Index.
Results
The mean age of the individuals participating in the study was 61.94 ± 10.34 years. According to the Pittsburgh Sleep Quality Index classification, 25.0% (n = 16) of individuals with diabetic foot ulcers had good sleep quality while 42.7% (n = 35) of individuals without diabetic foot ulcers had good sleep quality. A statistically significant relationship was found between diabetic foot ulcers and Pittsburgh Sleep Quality Index classification (p = 0.026). According to the multivariate logistic regression model, diabetic foot ulcers increased the risk of poor sleep quality by 2.64 times.
Conclusions
Our study showed that the presence of diabetic foot ulcers adversely affects sleep quality. Good sleep quality contributes to quality of life, wound healing, and diabetes control. Therefore, improving sleep quality in diabetic foot patients is important.
INTRODUCTION
Diabetic foot is one of the complications of diabetes that arises from motor, sensory, and autonomic neuropathy, macrovascular disease, skin infections, and mechanical factors [1]. Additionally, diabetic foot is a significant public health issue that can cause psychological, physical, social, and economic problems, affect quality of life, prolong hospital stays, and increase diabetes-related mortality and morbidity, leading to organ loss over time [2].
Sleep disturbance is a symptom that can stem from various physical and psychological factors and may affect anyone. As of now, there is no universally consistent theoretical definition of sleep disturbance. It is typically described as either poor sleep quality or abnormal sleep duration [3]. Sleep disturbances are recognized as a disruptive factor that promotes the onset and persistence of pathologies. Moreover, it has been observed that this disruption is bidirectional, meaning that treatments administered to patients with chronic conditions have a reduced impact when they also experience sleep disturbances [4].
The occurrence of sleep disturbance runs parallel to the high prevalence of diabetes [3]. In addition to directly causing sleep disturbances due to factors like nocturia, polyuria, diabetic neuropathy, and neuropathic pain, diabetes has also been linked to various chronic illnesses such as obstructive sleep apnea, cardiovascular complications, hypertension, cerebrovascular accidents, and depression. These conditions can further compromise both sleep and overall quality of life [5].
In recent years, the relationship between diabetes and sleep has become important, and research has shown that there is also a bidirectional relationship between sleep and diabetes: Diabetes can cause a decrease in sleep quality and sleep disturbances, while sleep disturbances can also make diabetes control difficult. Abnormal sleep duration, either shorter or longer than normal, can increase complication rates [6-8].
Having a good sleep process, one of the most important daily life activities, contributes to tissue renewal, repair of cell damage, and hormonal balance in individuals. At the same time, it improves the quality of life with its psychological and physical effects [2,9,10]. Therefore, sleep plays a crucial role in ulcer healing in diabetic foot ulcers (DFU).
In a comprehensive review study, no direct associations were identified between sleep quality and sleep duration concerning diabetic foot or diabetic foot ulcer variables. However, the study strongly advocates that future research, particularly randomized controlled trials, should explore interventions targeting sleep quality and sleep duration [11].
In this study, we aim to investigate the sleep quality of type 2 diabetic patients with and without foot ulcers, whether there is a difference in sleep quality between them, and the effect of DFU on sleep quality.
METHODS
A prospective cross-sectional study was conducted among insulin-using type 2 diabetes patients who applied to the Family Medicine Diabetes Clinic and Diabetic Foot Clinic of the Education and Research Hospital between April 1, 2021, and October 1, 2021. On March 15, 2021, with decision number HNEAH-KAEK 2021/102-3263, ethical approval was obtained from the Haydarpaşa Numune Training and Research Hospital Ethics Committee. Informed consent was obtained from all individual participants included in the study.
Participants
The minimum number of patients with diabetic foot diagnosis was determined as 64, and the number of diabetic patients without diabetic foot was determined as 82 when divided into strata using simple random sampling. A total of 146 patients who met the inclusion criteria were informed about the study and written and verbal consent was obtained. Diseases that affect sleep quality (psychiatric illnesses, metabolic disorders, active history of malignancy, sleep disorders including insomnia, parasomnia, sleep-wake disorder, sleep breathing disorder), use of medications that affect sleep quality (anticonvulsants, antidepressants, antipsychotics, xanthines, dopamine agonists, zopiclone, eszopiclone, zaleplon, zolpidem, benzodiazepines), and patients with a history of alcohol addiction (alcohol consumption > 20 g/day) were excluded from the study.
Process
A face-to-face interview was conducted with the patients to obtain sociodemographic data and information on HbA1c, waist circumference, diabetes duration, presence of diabetes-related complications (retinopathy, nephropathy, and neuropathy as microvascular, and ischemic heart disease, peripheral vascular disease, and cerebrovascular disease as macrovascular), lifestyle (smoking, alcohol use), and living environment (alone, with spouse or children, with caregiver) using a data collection questionnaire and the Pittsburgh Sleep Quality Index (PSQI). Those with a PSQI score >5 were considered to have poor sleep quality.
Waist circumference information was obtained through a physical examination, while HbA1c levels, diabetes duration, and the presence of diabetes-related complications were obtained through a review of electronic medical records.
Rating Scales
The PSQI was developed by Buysse et al. [12] in 1989, and its validity and reliability were assessed in Turkey by Ağargün et al. [13] in 1996. The PSQI is evaluated with seven component scores, each of which is scored between 0 (no difficulty) and 3 (severe difficulty). The component scores are summed to create an overall score between 0 and 21, with higher scores indicating worse sleep quality.
Statistical Analysis
The normal distribution of continuous variables such as age, waist circumference, HbA1c, diabetes duration, and PSQI was evaluated graphically and by the Shapiro-Wilk test. It was determined that none of the continuous variables, except for age and waist circumference, followed a normal distribution. Therefore, median (interquartile range) values were used to present descriptive statistics.
Independent samples t-test was used for the comparison of age, waist circumference, HbA1c, diabetes duration, and PSQI parameters that showed a normal distribution according to the presence of DFU, while Mann-Whitney U test was used for parameters that did not follow a normal distribution. Chi-square test was used for the comparison of categorical data.
Potential risk factors associated with PSQI classification were examined using multivariate logistic regression analysis. The results were presented as odds ratio (Exp(B)) and 95% confidence interval. IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY, USA) and MS-Excel 2007 programs were used for statistical analysis and calculations. The level of statistical significance was set at p < 0.05.
RESULTS
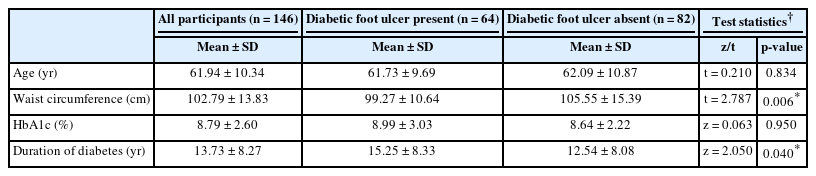
The mean age, HbA1c levels, and duration of diabetes of the study participants are shown in Table 1.
Comparison of parameters according to diabetic foot ulcer status
There was a statistically significant difference in waist circumference values among individuals based on their DFU status (t = 2.787, p = 0.006). Similarly, a statistically significant difference was found in the duration of diabetes values among individuals based on their DFU status (z = 2.050, p = 0.040) (Table 1).
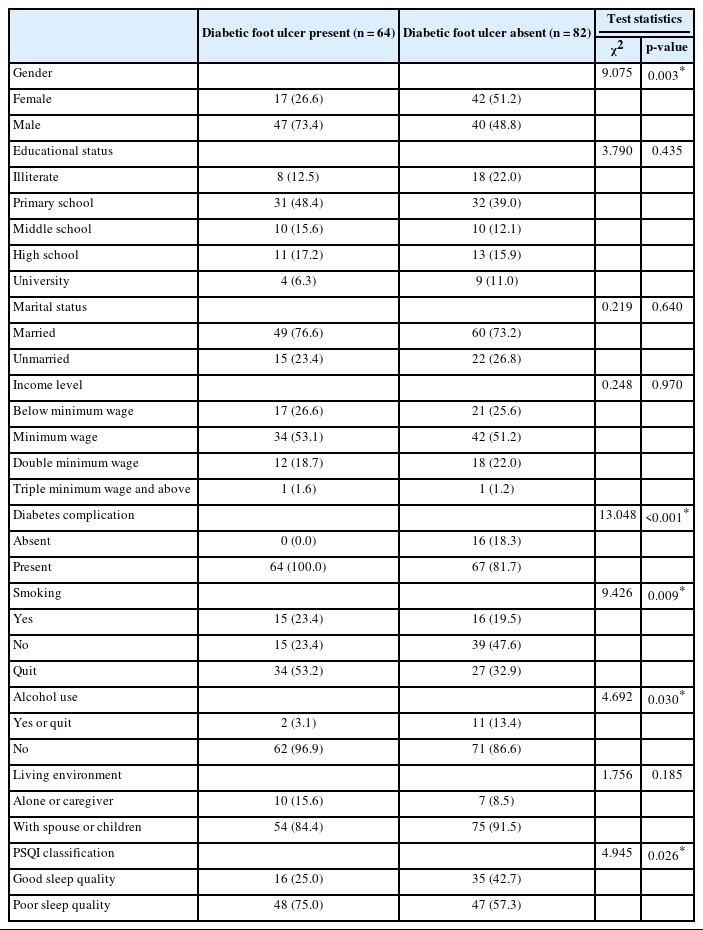
Of the participants with DFU, 26.6% (n = 17) were female, whereas 51.2% (n = 42) of those without DFU were female. A statistically significant difference was observed in the gender distribution according to the presence of DFU (χ2 = 9.075, p = 0.003). All individuals with DFU (n = 64) had diabetes complications, while 81.7% (n = 67) of those without DFU had diabetes complications. A statistically significant difference was found in the distribution of diabetes complications according to the presence of DFU (χ2 = 13.048, p < 0.001). Furthermore, statistically significant differences were found between the groups according to smoking and alcohol consumption (Table 2).
Distribution of responses to other variables according to individuals’ diabetic foot ulcer status
According to the PSQI classification, 25.0% (n = 16) of individuals with DFU had good sleep quality, while this rate was 42.7% (n = 35) for individuals without DFU. A statistically significant difference was observed in the distribution of PSQI classification according to the presence of DFU (χ2 = 4.945, p = 0.026) (Table 2).
The results of the multivariate logistic regression model that included the presence of DFU, gender, education, income, duration of diabetes, diabetes complication status, age, waist circumference, smoking status, alcohol consumption, HbA1c, and their effects on sleep quality are presented in Table 3 (Nagelkerke’s R2: 0.145). The presence of DFU predicted sleep quality with statistical significance (p = 0.032). The effect of DFU on sleep quality was found to be significant, whereas the effects of other variables on sleep quality were not statistically significant. DFU increased the likelihood of poor sleep quality by 2.64 times (Table 3). The Hosmer-Lemeshow test statistic was 6.64 with a p-value of 0.576.

Variables predicting sleep quality in multivariate logistic regression model
DISCUSSION
There are direct or indirect relationships between diabetes, diabetic foot, and sleep quality that affect each other. In a study conducted by Chao et al. [6], it was found that sleeping less or more than normal increases the risk of diabetes, while according to a study by Shaikh et al. [7], sleep deprivation affects the balance of leptin and ghrelin concentrations, appetite and insulin sensitivity. Diabetes can cause a decrease in sleep quality and sleep disturbances, while sleep disturbances can also make diabetes control difficult. Good sleep contributes to tissue regeneration, repair of cell damage, and individuals’ hormonal balance [2,9,10]. Therefore, sleep has a significant role in DFU and wound healing.
Song et al. [14] demonstrated a correlation between poor sleep quality and an elevated risk of developing type 2 diabetes mellitus (T2DM). The researchers highlighted that regulating sleep quality within an appropriate range could be a preventive measure for T2DM. The study conducted by Haveleia and Gayatri [15], which investigates sleep quality and influencing factors in patients with diabetic ulcers, revealed a significant difference between subjective sleep quality and sleep quality measured using PSQI. Additionally, the study found that pain and stress were significantly associated with poor sleep quality. In a study by Raman et al. [16] examining abnormal sleep patterns in individuals with T2DM and their impact on diabetic microangiopathies, lower daily sleep duration and quality were observed in patients with diabetic peripheral neuropathy. Conversely, a study by Sheahan et al. [17], focusing on differences in the daily activity of patients with DFU compared to controls in their free-living environments, indicated that the DFU group did not exhibit differences in lying down duration and sleep duration when compared to diabetic peripheral neuropathy and T2DM controls groups.
In a study conducted by Zhu et al. [18] on diabetics, the average PSQI score of patients was 8.30 ± 4.12, and it was found that sleep disorders adversely affect glycemic control. In a study by Selen and Polat [19], which involved 61 DFU patients, nocturia was found in 44.3% of patients, the average PSQI score of patients was 7.72 ± 3.38, and the sleep quality of 82% of patients was found to be poor. In a study by Salomé et al. [20], involving 60 patients with DFU, nocturia was detected in 80% of individuals, and poor sleep quality was found in 71.7% of individuals. In our study, poor sleep quality was found in 75% of individuals with DFU according to the PSQI classification, while poor sleep quality was detected in 57.3% of individuals without DFU. A statistically significant relationship was found between DFU and poor sleep quality. The observed relationship in our study could be attributed to poor glycemic control, pain, or stress in individuals with DFU.
According to the review conducted by Monteiro-Soares et al. [21], male gender was reported as a risk factor for the development of DFU. In the review, 34 studies evaluating the relationship between diabetic foot and gender were evaluated, and statistically significant results were obtained in 10 studies indicating a risk factor for male gender. In the study conducted by Demir et al. [22], 64.7% of 288 foot ulcers developed over an 8-year period occurred in men and 35.3% occurred in women. Similarly, in our study, the proportion of male patients with foot ulcers was higher in the patient group (73.4%).
The studies have shown that smoking and alcohol use are risk factors for diabetes, diabetic foot, and other diabetes-related complications [23,24]. Smoking can exacerbate diabetic peripheral sensory, autonomic, and motor neuropathy, which are important causes of foot ulcers. It leads to increased vasoconstriction, tissue hypoxia, and impedes the healing process [25]. Of the patients included in our study, 21.2% were active smokers, and 41.8% had quit smoking before. When we looked at the difference between the two groups, 76.6% of diabetic foot patients were active smokers or had quit smoking in the past, whereas this rate was 52.4% in non-diabetic foot patients. A statistically significant difference was found between the two groups regarding smoking status. In terms of alcohol use, individuals with diabetic foot consumed less alcohol due to social drinking, unlike the literature.
In the systematic review by Monteiro-Soares et al. [21], a relationship between diabetes duration and DFU was found in 25 out of 45 studies. Boyko et al. [26] examined the formation of DFU by monitoring 1250 diabetic patients every 3 months for an average of 3.3 years, and found a significant relationship between diabetes duration and foot ulcers. Pham et al. [27] also found a significant relationship between diabetes duration and foot ulcers in the study of 248 diabetic foot patients. In our study, the mean diabetes duration of individuals with DFU was 15.25 years, whereas the mean diabetes duration of individuals without foot ulcers was 12.54 years. A statistically significant relationship was found between DFU and diabetes duration values.
In the study by Porciúncula et al. [28], the mean waist circumference of DFU patients was found to be 99.3 cm, whereas it was determined as 107.4 cm in the non-ulcer group, and a statistically significant difference was detected. In a study by González et al. [29], which involved 89 type 2 diabetic patients with DFU and 109 patients without foot ulcers, no significant relationship was found between waist circumference and foot ulcers. When we compared the two groups in our study, the mean waist circumference of diabetic foot patients was 99.27 cm, whereas it was 105.55 cm in non-diabetic foot patients. A statistically significant difference was found between the two groups, and similar to the findings of Porciúncula et al. [28], it was found that the mean waist circumference of individuals without DFU was higher than that of individuals with DFU.
In the multivariate model that investigated the effect of diabetes-related variables, such as diabetic foot, gender, education level, income, diabetes duration, diabetes complication status, age, waist circumference, smoking, alcohol use, and HbA1c on sleep quality, the diabetic foot status of patients significantly predicted sleep quality. Diabetic foot increased poor sleep quality by 2.64 times. Our study found that diabetic foot patients and non-diabetic foot patients had different sleep quality levels.
Limitations
The primary limitation of our study is its cross-sectional design. Secondly, the absence of any classification for the evaluation of diabetic foot in our study can be considered a limitation. Thirdly, the lack of pain assessment in diabetic foot patients is another constraint.
Conclusion
Poor sleep quality was detected in 65.1% of diabetic patients included in our study. Poor sleep quality was observed in 75.0% of patients with DFU and 57.3% of patients without foot ulcers. A relationship was found between the presence of foot ulcers and sleep quality. It was determined that the presence of foot ulcers in type 2 diabetics increased the risk of poor sleep quality by 2.64 times. In addition to diabetic foot education, sleep hygiene education can also be provided to diabetics. It is appropriate to regulate the treatment of patients with poor sleep quality and severe sleep disturbances.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Author Contributions
Conceptualization: all authors. Data curation: all authors. Formal analysis: Eylem Suiçmez, Akın Dayan. Investigation: Eylem Suiçmez, Egemen Tural. Methodology: all authors. Project administration: all authors. Resources: all authors. Software: Eylem Suiçmez. Supervision: Eylem Suiçmez, Akın Dayan. Validation: all authors. Visualization: Eylem Suiçmez, Akın Dayan. Writing—original draft: all authors. Writing—review & editing: all authors.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Funding Statement
None
Acknowledgements
We extend our gratitude to all participants who contributed to this study.