Emotion Regulation Strategies as a Moderator Between Insomnia Severity and Bedtime Procrastination
Article information

Abstract
Background and Objective
Bedtime procrastination, defined as the behavior of going to bed later than intended in the absence of external factors, has been associated with insomnia and emotion regulation. The present study aimed to explore the moderating effect of emotion regulation strategies in the relationship between insomnia severity and bedtime procrastination.
Methods
This sample consisted of 374 adults (mean age 23.08 ± 2.17 years, 84.5% females). Participants completed the Bedtime Procrastination Scale, an Emotional Regulation Strategy checklist, and the Insomnia Severity Index.
Results
Bedtime procrastination was positively correlated with insomnia severity (r = 0.280, p < 0.001) and negatively correlated with active coping (r = -0.148, p < 0.01). Insomnia severity was positively correlated with avoidance coping (r = 0.099, p < 0.05) and negatively correlated with active coping (r = -0.170, p < 0.01) and support-seeking coping (r = -0.110, p < 0.05). There was a significant moderating effect of support-seeking coping in the relationship between insomnia and bedtime procrastination (B = 0.0165, 95% confidence interval = 0.0014–0.0316).
Conclusions
As a result of the present study, individuals using more support-seeking coping were more likely to delay bedtime as their insomnia symptoms became more severe. These findings suggest that support-seeking coping may be an important factor to consider in the clinical context of providing intervention for individuals with insomnia.
INTRODUCTION
Insomnia is a sleep disorder characterized by difficulty initiating or maintaining sleep accompanied with daytime function impairment [1]. Insomnia poses as a risk factor for various psychiatric symptoms [2,3], which have been partially explained by its link to sleep and emotion regulation difficulties [4,5].
Many theoretical models of emotion regulation have highlighted specific adaptive or maladaptive strategies that effectively reduce negative emotions [6-8]. The process model of emotion regulation developed by Gross [8] proposes that emotion regulation is conceptualized as a process that takes place throughout the unfolding of emotional responses. Based on this model, emotion regulation strategies can be categorized two strategies: antecedent-focused strategies and response-focused strategies [8,9]. In previous studies, suppression, one of the response-focused strategies, has been associated with decreasing positive emotions, weakened social support, and increased sympathetic activation of the cardiovascular system [9-11]. This result may suggest that using maladaptive emotion regulation strategies is a potential threat to sleep and health, considering many sleep disorders have exaggerated and maladaptive neurobiological and cognitive-emotional responses to stress [12]. Furthermore, individuals with insomnia may perceive bedtime as aversive due to staying awake for long periods of time at night [13], and their bedtime habits may be influenced by the strategies they take to regulate these negative emotions. For instance, individuals with insomnia symptoms may strategically delay their bedtime to avoid negative feelings to increase their readiness for sleep [14,15].
Bedtime procrastination is a sleep health behavior that is defined as “going to bed later than intended, without having any external factors for doing so” [16]. Bedtime procrastination has been shown to be associated with insufficient sleep and insomnia, as well as other psychological variables such as depression and anxiety [16-18].
Recent studies of procrastination have suggested that procrastination is associated with maladaptive emotion regulation strategies such as avoidance [19,20]. Similarly, previous studies have shown that individuals engage in bedtime procrastination by primarily engaging in smartphone use before bedtime [17,21,22] in an effort to regulate negative emotions [23-25]. Studies have found that individuals report using their phones before going to bed relieves stress [23] and distracts themselves from negative thoughts [14]. Furthermore, a previous study of bedtime procrastination by our research group conducted functional analysis of bedtime procrastination and found the main reported function of bedtime procrastination to be emotional regulation [15]. However, based on Gross’ model, not all emotion regulation strategies are effective [11]. Thus, it is necessary to explore what specific types of emotion regulation strategies are associated with the relationship between insomnia symptoms and bedtime procrastination, because the emotional experience of bedtime for individuals with sleep problem such as insomnia may differ from that of non-clinical populations.
For this reason, this study aims to explore the moderating effect of three emotion regulation strategies (active coping, avoidance coping, and support-seeking coping) in the relationship between insomnia severity and bedtime procrastination.
METHODS
Participants
The data for this study was collected as a part of a larger intervention study targeting individuals with high levels of bedtime procrastination [15]. Participants were recruited between March 2019 and March 2020 in Seoul, South Korea, using advertisements through online community postings and offline fliers. This study was approved by Sungshin Women’s University Institutional Review Board (SSWUIRB 2019-003). In this study, young adults were recruited based on the previous study that noted that general procrastination behavior was most common in early adulthood [26].
A total of 402 volunteers completed the online survey that recruited participants for this study. Among the respondents, 28 individuals who did not complete the online survey or had errors in responses to the survey were excluded from the study. A total of 374 participants were included for final analysis.
Measurements
Bedtime Procrastination Scale
The Bedtime Procrastination Scale (BPS) was developed by Kroese et al. [16] and measures the degree of bedtime procrastination. The BPS consists of 9 items that describe sleep-related behaviors and habits that reflect high or low level of bedtime procrastination. Items were rated on a 5-point Likert scale from 1 (almost never) to 5 (almost always). The BPS total score range is 9 to 45 points, with higher scores reflecting higher levels of bedtime procrastination. The Cronbach’s α was 0.72 in this study.
Insomnia Severity Index
The Insomnia Severity Index (ISI) was developed by Bastien et al. [27] and is composed of 7 items that measure the severity of insomnia during the past 2 weeks. The ISI is rated on a 5-point Likert scale from 0 to 4. The total score range is 0–28, and higher scores reflect greater insomnia severity. In the present study, participants who scored above 15 were excluded [28]. The Cronbach’s α was 0.64 in this study.
Emotional Regulation Strategy checklist
The Emotional Regulation Strategy (ERS) checklist developed by Yoon [29] is composed of 25 items that measure emotion regulation strategy of individuals. The emotional regulations strategy checklist is rated on a 5-point Likert scale from 1 to 5. The total score range is 25–75. This checklist contains three subscales as follows: 1) active coping (ERS_A): planning and taking specific strategies to solve problems; 2) avoidance coping (ERS_D): avoiding and distracting from problem situations; and 3) support-seeking coping (ERS_S): seeking emotional and instrumental social support from social relationships. The Cronbach’s α was 0.73 in this study.
Statistical Analyses
All statistical analyses were conducted by using SPSS Statistics version 21 (IBM Corp., Armonk, NY, USA). Correlational analyses were conducted using Pearson’s correlation coefficient between main variables.
The moderation effect was analyzed using Model 1 in PROCESS [30]. Analyses were bootstrapped with 5000 replications to calculate standard errors and 95% confidence intervals. A total of three models were constructed with the moderator based on three types of emotion regulation strategies (M). In all models, ISI was entered as the predictor (X) and BPS was entered as outcome (Y). The three modeled differed based on the types of moderating variable entered: ERS_A, ERS_D, and ERS_S. Simple slopes analysis was conducted on the moderating effects to detect relationships between the predictor and outcome variable at three levels of the moderator (low means one standard deviation [SD] below the mean; medium means mean, and high means 1 SD above the mean). Furthermore, the Johnson-Neyman technique [31] was conducted to determine which value ranges of the moderating variable the interaction (moderating) effect was statistically significant or not. Johnson-Neyman technique can analyze the significance regions where the simple slope of the dependent variable to the independent variable is significantly different from zero [32]. Thus, this technique allows us to obtain cutoff points of the moderator at which the effect of the independent variable on the dependent variable is statistically significant [33].
Post-hoc exploratory analyses were conducted on variables with significant effects. An independent samples t-test was conducted by dividing the sample into two groups based on total mean score.
RESULTS
Demographic Information
Demographic information is presented in Table 1. The sample consisted of 374 participants (mean age 23.08 ± 2.17 years, 84.5% female). Most participants were university students (81.3%) and almost all participants were single (99.7%).

Demographic characteristics of participants
Association Between Variables
Table 2 shows the correlations, means, and SDs of the three measures in the current sample. BPS was positively correlated with ISI (r = 0.280, p < 0.001) and negatively correlated with ERS_A (r = -0.148, p < 0.01). In addition, ISI was negatively correlated with ERS_A (r = -0.170, p < 0.01) and ERS_S (r = -0.110, p < 0.05).

Correlations, means, standard deviations of the insomnia severity, bedtime procrastination and emotion regulation strategies (n = 374)
ERS_S as a Moderator between ISI and BPS
Results of the moderation analysis are presented in Table 3. ERS_S was found to moderate the relationship between ISI and BPS, indicating that the association between ISI and BPS varied as a function of ERS_S (Fig. 1). However, the moderation effect of ERS_A and ERS_D were not significant.
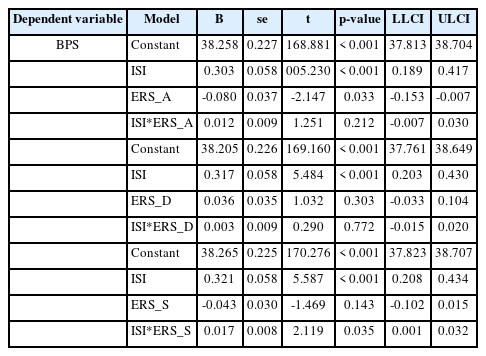
Moderating effect of emotional regulation strategies on the relationship between insomnia severity and bedtime procrastination (n = 374)
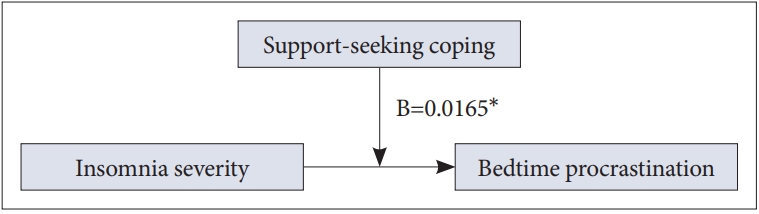
Model about moderating effect of support-seeking coping on the relationship between insomnia severity and bedtime procrastination. *p < 0.05.
Exploratory post-hoc analysis of the interaction was conducted by testing the conditional effects of an ISI at three levels of ERS_S, 1 SD below the mean, at the mean, and 1 SD above the mean (Fig. 2). ISI was significantly related to BPS at all three levels of ERS_S (coefficient1 SD below = 0.179, 95% CI = 0.009–0.348; coefficientmean = 0.343, 95% CI = 0.228–0.459; coefficient1 SD above = 0.442, 95% CI = 0.279–0.606).
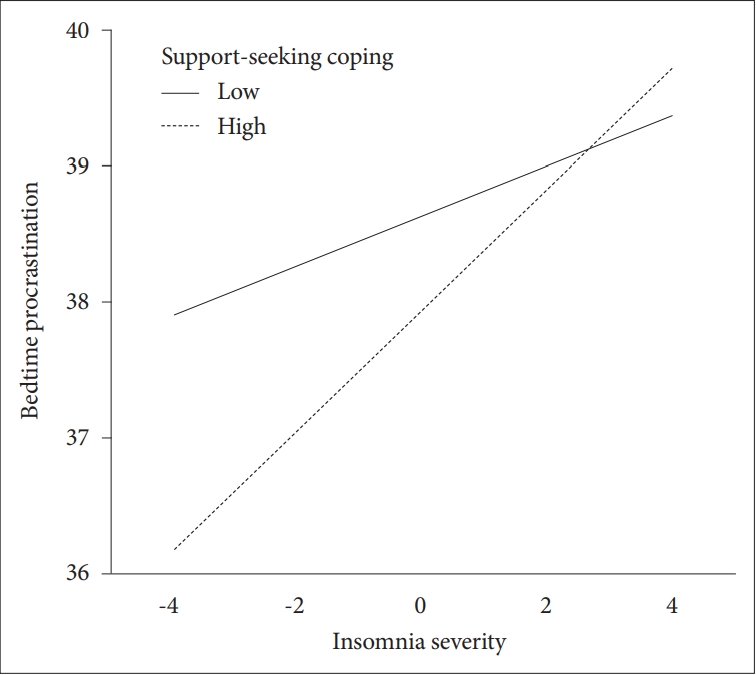
Moderating effect of support-seeking coping on the relationship between insomnia severity and bedtime procrastination.
Specifically, the significance region of the conditional effect of ERS_S was identified through Johnson-Neyman analysis (Table 4). The moderator value defining Johnson-Neyman significance region was -7.450, indicating that the conditional effect of ERS_S was significant when the score of ERS_S was higher than -7.450.

Support-seeking coping value defining Johnson-Neyman significance region
Independent Samples t-Test
Results of an independent samples t-test are presented in Table 5. The total sample (n = 374) was assigned to either the high-level ERS_S group (n = 213) or the low-level ERS_S group (n = 161) based on a total mean score of ERS_S (mean = 26.65). As a result, there were no significant different between the high-level ERS_S group (mean = 37.82, SD = 4.79) and the low-level ERS_S group (mean = 38.73, SD = 4.08) on BPS [t(372) = 1.925, p = 0.055].
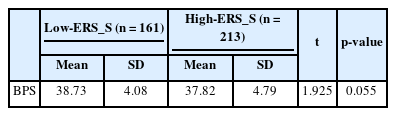
Association between support-seeking coping and bedtime procrastination (n = 374)
DISCUSSION
This study aimed to investigate the moderating effect of emotion regulation strategies on the relationship between insomnia severity and bedtime procrastination. The specific main results and implications are as follows.
Bedtime Procrastination as a Possible Emotion Regulation Strategy
Our results indicate insomnia severity was more strongly associated with bedtime procrastination in participants who endorsed support-seeking coping only, but not active or avoidant coping. To the best of our knowledge, this is the first study investigating the moderating effects of various types of emotion regulation strategies on the association between insomnia severity and bedtime procrastination.
Our findings are consistent with previous studies that insomnia and emotion regulation are associated with bedtime procrastination. According to a previous study, insomnia patients experience aversion to bedtime because the act of going to bed is repeatedly paired with restless, frustration for waiting to fall sleep [13]. These characteristics of insomnia symptoms may increase individual’s tendency for increasing time spent procrastinating before bedtime. Indeed, a recent study suggested that people who have difficulty falling asleep reported that they procrastinate their bedtime strategically [34]. In addition, some of these individuals report ruminating or feeling anxious if they do not fall asleep immediately, and postpone their bedtime to avoid having to deal with these negative emotions [34]. Therefore, people with insomnia may procrastinate their bedtime to reduce their negative emotions associated with not being able to sleep.
In our study, only support-seeking showed a moderating effect on the relationship between insomnia and bedtime procrastination. While these results are not consistent with previous studies that suggest procrastination is associated with emotion regulation strategies such as avoidance or active coping [19,20,35], our findings suggest that social interaction may be most associated with insomnia symptoms. Our results indicated the moderating effect of support-seeking coping was significant at all levels. However, participants with higher levels of support-seeking coping experienced greater increases in bedtime procrastination when insomnia symptom severity increased compared to participants with lower levels of support-seeking coping. These results suggest that individuals who utilize social resources more actively to escape negative feelings or thoughts may have stronger tendency to delay their bedtime when experiencing sleep problems such as insomnia.
However, it is unclear how support-seeking coping affects the relationship between insomnia severity and bedtime procrastination. One possible explanation may be that individuals who tend to engage in bedtime procrastination primarily use digital media devices before bedtime [17]. Mobile devices can facilitate engagement of social interaction even during the night and enhance perceived social support in those who prefer to engage in support-seeking coping. A previous study suggested that people who procrastinate at bedtime spend significantly more time on mobile applications for communication and leisure before bedtime [17]. Similarly, another previous study showed that participants use their digital devices to “post about feelings” and “seek someone out for help” [36]. Another possible explanation for our finding is that loneliness during nighttime may affect bedtime procrastination in individuals with insomnia. According to previous studies, the common experience of being awake for many hours alone in insomnia patients can lead to feelings of social isolation [37]. Although the relationship has yet to be fully understood, some studies reported that an increase in loneliness among younger adults is potentially related to their screen time and social media use [38]. Furthermore, it is possible that the emotion regulation coping strategies were partially influenced by the COVID-19 pandemic that occurred during the study period. During the pandemic, social interactions and support were limited and emotional distress increased [36]. Thus, participants may try to reduce their emotional distress or negative affect by engaging in indirect social interactions such as using social network services. In addition, the environmental changes that occurred because of COVID-19 may have also limited the emotion regulation strategies available to participants. A previous study found that emotion regulation strategies became more homogeneous after COVID-19 when the diversity of social and physical contexts experienced by participants was reduced [36]. Although only 76 of the 374 participants were recruited after the COVID-19 pandemic, restricted social support and limited diversity of emotion regulation strategies during this particular period may have influenced individuals to delay bedtime using support-seeking coping. However, it is also unclear whether delaying bedtime to gain social support is ultimately adaptive or maladaptive for individuals with insomnia symptoms. Although support-seeking coping is generally thought to be adaptive [39], recent studies suggest that social media-based support-seeking coping may lead to negative effects, termed “social media service (SNS) fatigue” [40]. Therefore, in future research, it is worth exploring the specific pathways and results that support-seeking coping influence the relationship between insomnia severity and bedtime procrastination.
Limitations and Recommendations for Research
This study has some limitations. First, our sample consisted of mainly females, and additional studies with higher proportion of male participants should be conducted to generalize our results. Second, the COVID-19 pandemic occurred during the period of our study. In our study, 76 of the 374 participants were recruited after the COVID-19 pandemic started. The COVID-19 pandemic dramatically changed social behaviors of individuals worldwide. In particular, lockdowns due to COVID-19 have led to an increase in social media use, and psychological problems such as loneliness and isolation have emerged as important mental health issues. These changes may have influenced our participants to seek more social support and use digital devices in bed for longer periods, overstating our findings. Therefore, future studies should be conducted to exclude special situational factors such as COVID-19. Third, the current study did not exclude psychopathological disorders such as depression, schizophrenia, and bipolar disorder because it was an exploratory study investigating the interaction of insomnia and emotion regulation strategies on bedtime procrastination. These disorders may affect participants’ sleep and mood. Therefore, it needs to exclude psychopathological disorders in future studies. Finally, this was an exploratory study that investigated the moderating effects of three different emotion regulation coping on the relationship between insomnia severity and bedtime procrastination. Thus, it did not investigate how the support-seeking coping that was shown to moderate the relationship between insomnia severity and bedtime procrastination affected the psychosocial adaptation. Therefore, future research should explore the specific processes by which support-seeking coping influences the relationship between insomnia severity and bedtime procrastination. In addition, it would be meaningful to determine what the consequences of bedtime procrastination associated with the use of support-seeking coping are for an individual’s sleep and psychology.
Conclusion
Despite these limitations, this study has the following contributions. First, this is the first study to investigate the interaction of insomnia and emotion regulation strategies on bedtime procrastination. To date, research on bedtime procrastination has been focused on how it affects sleep problems such as insomnia. However, bedtime procrastination likely occurs not only among healthy individuals but also among those who already experience insomnia. Considering that people with already experienced sleep problems are more vulnerable in terms of emotional and physical health compared to healthy individuals, it is important to understand what factors reinforce problematic behaviors such as bedtime procrastination in this population. Therefore, the present study is notable in that it is the first to investigate the impact of insomnia on bedtime procrastination and the role of specific emotion regulation strategies that are relevant in this relationship. Second, the present study found that the use of support-seeking coping was a significant factor influencing bedtime procrastination in individuals with insomnia. These findings suggest that social connections may be a key determinant of delayed bedtime for individuals experiencing sleep problems. Examining social relationships or lack of intimacy may provide a clinical context for delivering sleep interventions, especially for individuals who are likely to delay their bedtime.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Authors’ Contribution
Conceptualization: all authors. Data curation: Huisu Jeon. Formal analysis: Huisu Jeon, Wooyoun Lee. Funding acquisition: Sooyeon Suh. Investigation: Huisu Jeon. Methodology: Huisu Jeon. Project administration: Sooyeon Suh. Resources: Huisu Jeon. Software: Huisu Jeon. Supervision: Sooyeon Suh. Validation: Sooyeon Suh. Visualization: Huisu Jeon, Wooyoun Lee. Writing—original draft: Huisu Jeon, Wooyoun Lee. Writing—review & editing: Sooyeon Suh.
Conflicts of Interest
Sooyeon Suh, a contributing editor of Sleep Medicine Research, was not involved in the evaluation process or decision to publish this article. The remaining author has declared no conflicts of interest.
Funding Statement
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2018S1A5A8026807).
Acknowledgements
We thank Sonhye Jeoung, Hyeyoung An, Goeun Kim, and Hyojin Nam of the Department of Psychology, at Sungshin University who provided assistance for this study.