Sleep Patterns, Insomnia, and Well-Being Among Female High School Students: A Population-Based Study
Article information

Abstract
Background and Objective
The role of insomnia in the well-being of school children has not been sufficiently examined in the literature. We aimed to explore the prevalence of clinical insomnia and its relationship to the health-related quality of life among female high-school students.
Methods
In a cross-sectional study in 2018, 300 students from five female high-schools in the Kurdistan Region were randomly included, regardless of age and other socio-demographic characteristics. The Personal Wellbeing Index, General Health Questionnaire–12, and Insomnia Severity Index were used to measure the personal and general well-being, and insomnia of school children, respectively.
Results
The students were categorized into short sleepers (2.0%), normal sleepers (51.0%), and long sleepers (47.0%), and age range is 14–19 years (mean: 16.22 years). The mean value of general well-being and insomnia severity was 6.89 and 11.42, respectively. We found that 25.0% of the students had no clinically significant insomnia, 47.7% had subthreshold insomnia, 24.0% had clinically moderate insomnia, and 3.3% had clinically severe insomnia. The mean value of the personal well-being of students was 7.91 out of 10. The mean value of personal well-being was significantly lower among students with more severe insomnia. The mean values of personal well-being were 8.61 (no clinically significant insomnia), 7.87 (subthreshold insomnia), 7.49 (clinically moderate insomnia), and 6.91 (clinically severe insomnia). The worse sleep situations and smoking were the main independent controlling factors for lower personal well-being.
Conclusions
The study documented that female students are at risk of being clinical insomniacs, and are at risk of the development of lower well-being.
INTRODUCTION
Insomnia is considered a major health issue among the general population. The prevalence of insomnia has increased worldwide [1]. Insomnia is characterized by repeated difficulty with the initiation, maintenance, consolidation, or quality of sleep. This situation occurs despite sufficient time and opportunity for sleep and leads to daytime impairment. There are different criteria for insomnia, but we focus on the common one in this paper: that of the individuals who take > 30 min to fall asleep, stay asleep for < 6 h, wake > 3 times at night, or experience sleep that is chronically nonrestorative or poor in quality. It has been reported that roughly one-third of the adult population have had some difficulty falling asleep and/or staying asleep during the previous year. In this regard, 17% of the population report the sleep issue as a main problem in their lives, and between 9% and 12% experience daytime symptoms. Interestingly, 15% of them are dissatisfied with their sleep, 6%–10% meet the diagnostic criteria for insomnia syndrome [2].
Different prevalence rates of insomnia have been reported in the literature by observational studies. A population-based cross-sectional study of teenagers aged 16 to 18 in western Norway discovered that 65% reported sleep onset latency that was longer than 30 min. In their investigation, women revealed a greater prevalence of insomnia than men, and a longer sleep start latency. However, the boys did report later bedtimes and a larger weekday–weekend difference in a number of sleep-related variables. The prevalence of insomnia ranged from 23.8% (based on the Diagnostic and Statistical Manual of Mental Disorders, 4th edition [DSM-IV] criteria), through 18.5% (based on the DSM-5 criteria), to 13.6% (quantitative criteria for insomnia) [3].
A similar issue has been reported in other developed countries as well, for example, 34.6% of adolescents in Australia [4] and 38.1% in the USA indicated 34.8% short sleep duration (< 7 h) and 83.1% long sleep onset latency (≥ 30 min) [5]. Sleep problems among adolescents have been reported in developing countries as well, for example, 46% sleep deprivation (< 7 h) on weekdays and 33% on weekends in Saudi Arabia [6], 59.6%, 29.5%, and 12.1% insomnia, daily sleepiness, and sleep deprivation, respectively, among Egyptian youths [7]. In terms of our region, there has been no previous study of school children. But the prevalence of insomnia among medical university students is 25% [8]. The studies have reported that female students are more at risk of insomnia compared to males in high schools. For example, Hysing et al. [3] showed that the female sex has a significant association with insomnia. The pooled prevalence rate of insomnia among the general population is 22.0%. It has been reported that in a meta-analysis of 13 observational studies, females have a significantly higher prevalence rate of insomnia compared to males [1].
Insomnia, owing to its chronic nature, is responsible for several negative outcomes. Some of these negative outcomes are impaired daily functioning, poor mental health, and lower quality of life [9]. Mental illness is the most common disease among the general population burdening all conditions [10]. Mental illnesses, such as depression and anxiety, are common, not only among older adults, but are also common across the entire human lifespan. But late childhood and adolescence are crucial developmental periods in mental health issues and general well-being, along with other psychiatric issues; these include anxiety disorders, mood disorders, eating disorders, and psychosis. These mental illnesses are frequently chronic and recurrent. The onset of these mental illnesses at earlier ages is related to a more severe and resistant course, crucial impairments to educational and social functioning, and reduced quality of life [11].
Research Problem and Aim
A person’s health is impacted by insomnia in a number of different ways. When the brain circuitry does not receive the right amount of sleep, poor sleep impacts the brain’s ability to function properly. It is unable to save or retrieve data, or maintain high levels of performance while under stress [12]. The serious health risks associated with insomnia according to the National Institute for Health include the following: medical conditions (obesity, high blood pressure, weak immune system, diabetes mellitus, heart disease, sensitivity to pain, stroke), mental health disorder (risk of depression, poor memory, slowed reaction time, risk of anxiety disorder, incoordination), and increased risk of accidents (motor vehicle accident because of fatigue–sleep-deprived drivers) [12]. A study included 1.1 million men and women aged 30–102 years old. The best survival rate was found among those participants who slept 7 h per night. The persons who sleep ≥ 8 h experience significantly higher mortality hazards, compared to those persons who sleep < 6 h. “The increased risk exceeded 15% for those reporting more than 8.5 hours sleep or less than 3.5 or 4.5 hours” [13].
The individual and the student of high school stage require sufficient sleep to meet the student’s need for attention, memory, and good health. School children are considered the most important layer of each society. The study on insomnia and its association with general and personal well-being has not been sufficiently investigated among school children. The present study aimed to explore the prevalence of clinical insomnia and its relationship with the health-related quality of life among female high school students.
METHODS
Study Design and Sampling
A random sample of female schoolchildren from 15 secondary schools was included in this cross-sectional study. The researchers numbered the 15 secondary female schools consecutively. Among these 15 schools, five were randomly selected through a simple random sampling technique by digit number chart. Each school had between 10 and 12 classes. We randomly selected five classes from each school, again through simple random sampling. The number of students in each class was between 40 and 50 students. In this regard, we selected 12 students through a simple random sampling based on the pre-generated random sampling list; the students were numbered from 1 to 50 and selected students were invited to participate in this study. Finally, we included 300 students in this study through a multistage random sampling technique in 2018.
Setting and Study Process
The study was conducted in Duhok city in Kurdistan Region in 2018. We obtained the list of available female high school students from the General Directorate of Education in Duhok city. We included all 15 available female high schools in the randomization process. We selected five female high schools in this study. The selected schools were reviewed in terms of geographic areas. The schools were from different geographic areas, including areas with low and high sociodemographic characteristics. In addition, the morning and evening high schools were included in this list. We intended to repeat the randomization process in the case of selecting more schools in one geographic area. The Duhok governorate is one of the four official governorates of the Kurdistan Region in Iraq.
Sample Size
The sample size was determined using the Cochran formula (
Inclusion and Exclusion Criteria
The participants were female students in high school aged between 13 and 18 years old who, regardless of their socio-demographic characteristics, were eligible to participate in the study. The students who were absent during data collection or did not show interest in participating, were excluded from the study. In addition, mixed high school students were not included in this study, due to the difficulty of selecting random participants.
Measurement Criteria
The information on the school children was recorded in a pre-designed questionnaire. The questionnaire collected the following information from the school children.
Socio-demographic characteristics
The general information of the student, including age; physical activity and its patterns; smoking and its types; smoking duration by year; and sleeping hours were obtained through the self-reported technique.
Personal well-being scoring
The Personal Well-Being Index–School Children (PWI-SC) scale has 7 questions, with each of them having 10 degrees. On this scale, 0 means that a person feels very sad, 10 means that a person feels very happy, and the middle of the scale is 5, which means that a person feels neither happy nor sad [14]. The Cronbach’s alpha for the entire set in this study was 0.6353.
General well-being
The general mental well-being of schoolchildren was measured by the General Health Questionnaire–12 (GHQ-12). The questionnaire has 12 items to measure healthy functioning and the onset of new distressing symptoms. The symptoms of the scale are associated with anxiety, depression, somatic symptoms, and social dysfunction. It is suitable for a wide age range [15]. The higher scores indicate the worse general well-being of the participants. The items are rated using a 4-point Likert scale, and summed to obtain a score between 0 and 36. The Cronbach’s alpha for the entire set in this study was 0.6685.
Insomnia Severity Index
The Insomnia Severity Index (ISI) has seven questions and is summed to get a total score. On this scale, the scores 0–7 are considered no clinically significant insomnia, 8–14 are considered subthreshold insomnia, 15–21 are considered clinically moderate insomnia, and 22–28 are considered clinically severe insomnia [16]. The Cronbach’s alpha for the entire set in this study was 0.6755.
Reliability and Validity
We utilized previously validated scales to measure personal and general well-being, as well as insomnia severity in this study. To ensure reliability, an independent author (other than the names of authors who were included in this study) translated the aforementioned scales into the Kurdish language. The Kurdish scales were then translated into English by the fifth author in collaboration with a colleague from the University of Duhok. Minor differences were found between the original English and the translated English scales. We also assessed the reliability of the Kurdish scales by calculating the Cronbach’s alpha of the first 20 questionnaires that were included in the study. The study proceeded once the obtained alpha Cronbach’s alpha was greater than 0.6. It is worth mentioning that the PWI-SC, GHQ-12, and ISI have previously been adapted for use among school children.
Bias Reduction Techniques
To minimize measurement bias in this study, all researchers convened for a meeting to discuss each question of the scales in detail. We commenced data collection only after achieving a consensus on the interpretation of all items of the scales.
Statistical Methods
The general characteristics of school children were presented in mean and standard deviation or number and percentage. The prevalence of insomnia was determined in number and percentage. The status of personal well-being, general well-being, and insomnia was determined by mean and standard deviation. The comparisons of personal well-being and general well-being among female school children with different sleep severities were examined by one-way analysis of variance. The pairwise comparisons of personal and general well-being between students with different insomnia severities were examined by Tukey test. The predictors of the personal well-being of students were examined in a standard square least with effect leverage. The null hypothesis was rejected with a p-value < 0.05. The statistical calculations were performed by JMP Pro (version 14.3.0; https://www.jmp.com/en_us/home.html).
Ethical Considerations
The ethical approval of the present study was obtained from the Scientific Research Division, Department of Planning of the General Directorate of Education in Duhok. The protocol of the study was registered on February 9, 2017 as reference number: 09022017-2. A guarantee of the confidentiality of their personal information was given to the students, and their participation was completely optional. We obtained administrative permission from the Duhok Directorate of Education and the school administrations and verbal consent from the children prior to data collection.
RESULTS
The mean age of the student was 16.22 (range 14–19) years. The mean value of family members was 8.16 (range 2–15) persons. Most of the students were physically active (67.67%), with an irregular pattern (67.98%). The majority of the students were nonsmokers (94.33%). The study found that the students were short sleepers (2.0%), normal sleepers (51.0%), and long sleepers (47.0%) (Table 1).

General characteristics of female high school students
The mean value of general well-being and insomnia severity in school children were 6.89 and 11.42, respectively. The study showed that 25.0% of the students had no clinically significant insomnia, 47.7% had subthreshold insomnia, 24.0% had clinically moderate insomnia, and 3.3% had clinically severe insomnia. The mean value of the personal well-being of students was 7.91 out of 10 (Table 2).
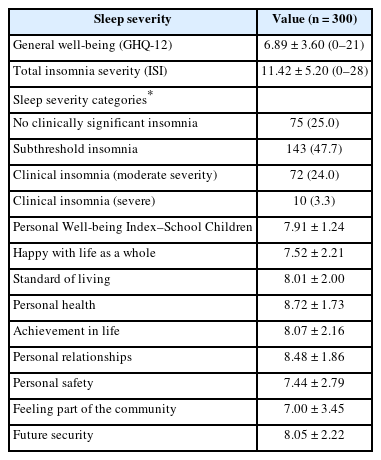
General well-being, personal well-being, and sleep severity among female high school students
The study showed that a considerable percentage of the female students had difficulty falling asleep (moderate: 21.67%, severe: 24.33%, and very severe: 22.67%) and difficulty staying asleep (mild: 33.00%, moderate: 23.67%, and severe: 10.33%). In addition, some students had problems waking up too early (mild: 21.67%, moderate: 15.67%, and severe: 7.67%). We found that 13.33% and 15.00% were not satisfied and very dissatisfied with the sleep pattern, respectively. The students believed that the sleep problem impaired their quality of life (somewhat: 17.67%, much: 20.33%, and very noticeable: 15.00%). The students were worried or distressed with their current sleep problem (somewhat: 16.00%, much: 10.67%, and very noticeable: 7.67%). The students reported that sleep problems interfere with their daily functioning, such as daytime fatigue, mood, ability to function at work/daily chores, concentration, memory, mood, etc. (somewhat: 22.00%, much: 17.33%, and very noticeable: 21.00%) (Table 3).

Prevalence of insomnia components among female school children
The study showed that the mean value of the personal well-being of school children was significantly lower among students with more severe insomnia. The mean values of personal well-being were 8.61 (no clinically significant insomnia), 7.87 (subthreshold insomnia), 7.49 (clinically moderate insomnia), and 6.91 (clinically severe insomnia). The pairwise comparisons analysis showed that students with subthreshold and clinically moderate and severe insomnia had significantly lower personal well-being, compared to the students with no clinically significant insomnia (Table 4 and Fig. 1).
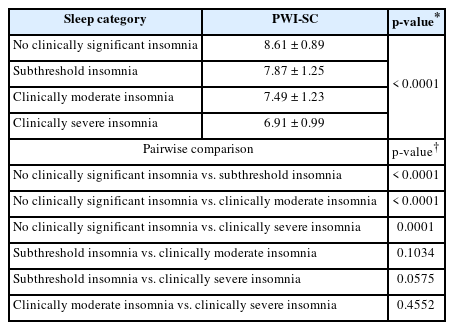
Comparisons of personal well-being among female school children with different sleep severity

Personal well-being of students with different insomnia severity. PWI-SC, Personal Well-Being Index—School Children.
The study showed that students with different insomnia severities had significantly different general well-being values. The students with subthreshold insomnia, clinically moderate insomnia, and clinically severe insomnia had significantly worse general well-being, compared to the students with no clinically significant insomnia. In addition, the students with clinically moderate insomnia had worse general well-being, compared to those students with subthreshold insomnia (Table 5 and Fig. 2). The study showed that worse sleep situations and smoking are the main independent controlling factors for lower personal well-being among female school children (Table 6).
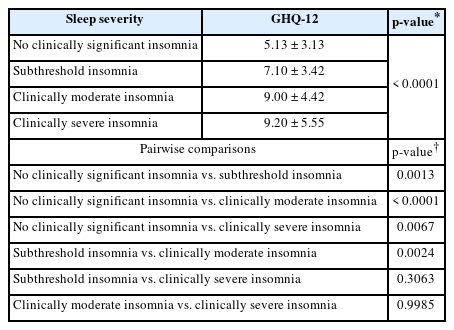
Comparisons of general well-being among female school children with different sleep severity

General well-being of students with different insomnia severity. GHQ-12, General Health Questionnaire–12.

Predictors of personal well-being of female school children
DISCUSSION
This study showed that subthreshold and moderate insomnia was high among female school children in Kurdistan region, and the children with more severe insomnia severity had worse personal well-being. Also, worse insomnia and smoking were identified to be the main controlling factors of personal well-being among female school children.
The role of insomnia in the general well-being and mental health status of children has been investigated in the literature. In this regard, a systematic review and meta-analysis examined the relationship between sleep disturbance and depression among adolescent populations. The study showed that depressive adolescents experience substantially more wakefulness in bed. The sleep issues experienced by depressive adolescents are sleep onset latency, waking after sleep onset, number of awakenings, and sleep efficiency. Additionally, insomnia has been shown to be associated with lighter sleep and more sleep disturbance among different populations. Sleep disturbance may be a precursor to the development of depression [17]. Puberty is a marker for the development of both depressive symptoms and sleep issues. Some sleep issues have been associated with puberty, including a delay in the timing of the circadian system, such as a delayed sleep period [18,19]. In this study, we found that older student age is an independent factor for lower general well-being. Also, we found that older age is a controlling factor for more sleep severity. The delay in sleep timing is responsible for sleep onset latency, and makes an opportunity for wakefulness in bed. This increased wakefulness in bed improves ruminative thinking styles, and later perpetuates further sleep disturbance [20,21]. The role of age in escalating insomnia has been reported elsewhere [22].
According to cohort studies, frequent night awakenings are linked to mental health conditions, such as affective symptoms, emotional difficulties, conduct issues, hyperactivity/inattention concerns, and mood and behavioral problems. The result is hyperactivity or inattention, which is connected to sleep habits. There is evidence linking a longer sleep onset latency and later bedtimes at school to a higher risk of emotional and behavioral problems [23]. We included female schoolchildren only in this study. It seems that among males, poor sleep is an external status, while among females, an internal one [23]. The literature has proved that sleep deprivation poses a modulatory influence on the onset of psychiatric conditions, including depression and emotional regulation among adolescents [24]. The new onset of sleep disturbance or persistent sleep disturbance has been reported to be a risk factor for the development of poorer mental health among Japanese junior high school teenagers [25]. In our study, problems waking up too early and difficulty falling asleep were predictors of the worse personal well-being of school children. Late bedtime has been associated with mental health disturbances like depression, anxiety, and suicidal or self-injury risk among twin adolescents [26].
It has been proved that sufficient sleep passively improves memory, skills, learning, and the extraction of knowledge [27,28]. The students with better sleep quality and quantity have more achievements among college students [8,29]. In addition, better sleep supports school-age children functionally [30]. Even one-night sleep deprivation negatively impacts neurobehavioral performance-attention, reaction time, and cognitive processing speed. Therefore, sleep deprivation poses adolescents at risk of the development of poor academic performance [31], impairs procedural and declarative learning [29], decreases alertness [32], impairs memory consolidation [33], and affects attention and decision-making [34].
Smoking has been significantly associated with insomnia and a high risk of obstructive sleep apnea in an Egyptian study as well [7]. The possible reason may lie in the correlation of age with general well-being. The general well-being of students significantly escalated with increasing age.
Strengths and Limitations
The strong point of this study is that we included the students through a random sampling technique. But the study was not exempt from limitations. We included only female schoolchildren in this study. Therefore, the study cannot be representative of all school children. Also, a cross-sectional study may not infer the causal pathway between insomnia and personal well-being. We did not include mixed high school students in this study.
Conclusions
This study showed a considerable percentage of female schoolchildren have clinical insomnia with different severities. In addition, a considerable percentage of school children had difficulty falling asleep, difficulty falling asleep, and problems waking up too early, and of sleep interfering with daily functioning. In addition, the study documented that those with moderate and severe levels of clinical insomnia had a lower score in personal well-being indicators. Worse sleep quality and smoking were determined to be the main predictors of worse personal and general well-being.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Authors’ Contribution
Data curation: Zakya Ageed Tufeq, Aziza Mohammed Ziyab, Bushra Abdulla Ahmed, Mohmmed Khuder Nafea Rahho. Formal analysis: all authors. Funding acquisition: Deldar Morad Abdulah. Investigation: Zakya Ageed Tufeq, Aziza Mohammed Ziyab, Bushra Abdulla Ahmed, Mohmmed Khuder Nafea Rahho. Methodology: Zakya Ageed Tufeq, Aziza Mohammed Ziyab, Mohmmed Khuder Nafea Rahho. Project administration: Deldar Morad Abdulah. Resources: Deldar Morad Abdulah. Software: Deldar Morad Abdulah. Supervision: Deldar Morad Abdulah. Validation: Deldar Morad Abdulah. Visualization: Deldar Morad Abdulah. Writing—original draft: Zakya Ageed Tufeq, Aziza Mohammed Ziyab, Bushra Abdulla Ahmed, Mohmmed Khuder Nafea Rahho. Writing—review & editing: Deldar Morad Abdulah.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Funding Statement
None.
Acknowledgements
The authors of this study would like to express their gratitude to the General Administration of Education, and to the high schools in Duhok city.
