Factors Associated With Sleeping Quality and Behaviors Among University Students in Malaysia
Article information

Abstract
Background and Objective
Sleep is an important physiological process for humans. Students of tertiary institutions, especially those at the university, are often reported to have poor sleep quality due to changing social opportunities and increasing academic demands. This study aimed to investigate the prevalence of poor sleeping quality and its relationship with academic performance and psychological distress among university students in Malaysia.
Methods
An online questionnaire-based, cross-sectional study was conducted among students of tertiary institutions in Malaysia. The questionnaire consisted of respondents’ demographics, Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), Horne-Ostberg Morningness-Eveningness Scale (MES) and Depression-Anxiety-Stress Scales (DASS-21). Simple and multiple linear regression were used to identify the relationship between the independent and dependent variables (PSQI score and MES score).
Results
Of the 403 respondents, about three-fourths were poor-quality sleepers. The cumulative grade point average (CGPA) was the only factor with a significant linear and positive relationship with the PSQI score. Only the depression and anxiety scores showed a significant linear and positive relationship between the PSQI score and the MES score.
Conclusions
Poor sleep quality was prevalent among university students. Poor sleep was associated with better academic performance. Students with depression or anxiety were significantly associated with poor sleep quality and being a morning bird.
INTRODUCTION
Sleep plays a vital role in our life as we generally spend one-third of our life sleeping. Thus, having a pleasant sleeping quality is paramount to guarantee life satisfaction. A good sleeping quality does not mean that the longer the duration, the better, it is influenced by the extent of the mind and body to attain restfulness [1].
Amidst one of the most critical phases of life, more than half of the tertiary institution students around the globe are found to have a poor quality of sleep, whereby researchers disclosed that 55.8% of undergraduate students in Ethiopia, 50.1% of undergraduate students in a Nigerian university, and also 55.9% of Peruvian undergraduate students had poor sleep quality [2-4]. In Malaysia, as high as 70.6% of undergraduate students in the local universities suffer from poor sleep quality [5]. A recently published study showed that 3 in 5 undergraduate health sciences students at a local university had poor sleep quality [6]. Seeing the high prevalence of unsatisfactory sleep quality, we need to fathom the contributing factors of this situation.
One of the common factors leading to poor sleep quality is using electronic devices such as laptops, mobile phones, and tablets before sleep. The use of mobile phones right before sleeping is found to increase sleep onset and repeated awakenings during sleeping [7]. Electronic device users may be exposed to more light generally, which could reduce the release of melatonin, a hormone that promotes sleep but is suppressed by light [8]. Another factor would be using caffeinated drinks, especially when overconsumed, to deal with daytime sleepiness because of poor sleep quality. It is a vicious cycle, as excessive consumption of caffeinated drinks would further worsen the sleep quality in caffeine-sensitive individuals [9]. Furthermore, another easily overlooked factor would be the existence of roommate (or roommates). A study investigating the effects of the sound environment on the sleep of Chinese college students concluded that the most common perceived sources of a noise interrupting sleep were roommate conversations, a collision of objects, furniture, door, and footsteps in the bedroom. The same study mentioned that the lower the number of occupants in a dorm, the higher the chances that the students would get enough sleep [10].
Finally, varying daily schedules might impact sleep quality as well. Schedule variability was higher among American college students with poor sleep quality than among those with good sleep quality. According to the same study, college students who have a noticeably delayed sleep-wake cycle are particularly vulnerable to experiencing poor sleep quality [11]. Speaking of social interaction, one may assume that students who participate in more social activities must compromise the quality of their sleep. Unexpectedly, Carney et al. [11] discovered that poor sleepers are those with less socially active lifestyles. This could be due to their being free to eat, sleep, or play any time they want, going against social conventions. Unlike when they are with their companions, in which there is more restrictive variability [11].
The academic performance and psychological health of tertiary institution students may suffer from poor sleep quality. Sufficient, high-quality sleep optimizes memory processing and learning. Sleep helps to sustain concentration, executive cognitive functions, and sensorimotor integration [12]. Sleep disturbance is a common sign of depression, and research has found a strong link between psychiatric problems and poor sleep [8]. A study of Thailand undergraduates revealed that students with poor-quality sleep had significantly increased negative moods such as anger, depression, and tension [13]. Realizing how university life might shape the sleep hygiene and mental states of the future pillars of the nation, we hypothesized that university students in Malaysia who have poor sleeping quality and behaviors are likely to have lower academic performance and experience psychological distress. The current study aimed to determine the prevalence and factors associated with poor sleeping quality and behavior among university students in Malaysia.
METHODS
Study Design
The study was an online cross-sectional study involving students of tertiary institutions in Malaysia using a semi-structured questionnaire via Google Forms. The online Google Forms were spread through many social media platforms, such as WhatsApp, Facebook, and email, to reach out to students from tertiary institutions all over Malaysia.
Participants
The study was conducted using a non-probability sampling technique, where the participants were selected through convenience sampling. The inclusion criteria for the study were tertiary institution students in Malaysia, aged 18 and above.
Study Instrument
The questionnaire consisted of five parts, where Part I consisted of respondents’ demographics and their cumulative grade point average (CGPA) as an indicator of their academic performance. A CGPA is a measure of a student’s overall academic performance over a period, typically an academic year or an entire course of study (all completed semesters). The CGPA was calculated by taking the average of the grade points obtained in all of a student’s courses. Each course was assigned a grade point based on the grade obtained in that course. The grade point for a course was typically calculated by multiplying the grade obtained by the credit hours assigned to the course. The grade points for each course were totaled together and divided by the total number of credit hours taken to determine the CGPA. The higher the CGPA, the better the student’s academic performance. Part II consisted of the Pittsburgh Sleep Quality Index (PSQI). The PQSI was used to differentiate between individuals with poor or good sleep quality by measuring seven aspects: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleep medication, and daytime dysfunction over the past month [14]. The questionnaire consists of 19 questions, which are weighted and scored to give a total score ranging from 0 to 21, with higher scores (5–21) indicating poor sleep quality and lower scores (0–4) indicating good sleep quality. Part III consisted of the Epworth Sleepiness Scale (ESS) to determine the general level of daytime sleepiness of an individual by a rating system that comprised eight different situations in which the person would doze off by using a scale ranging from 0 (would never doze) to 3 (high chance of dozing) [15]. Part IV consisted of the Horne-Ostberg Morningness-Eveningness Scale (MES) to evaluate the ‘chronotype’ or sleeping habits of an individual by summation of scores and converting them into scores in the MES: definitely morning type (70–86); moderately morning type (59–69); neither type (42–58); moderately evening type (31–41) and evening type (16–30) [16]. Parts II to IV of the questionnaire were adapted directly from a local study by Lai and Say [17]. The last part of the questionnaire, Part V, consisted of the Depression-Anxiety-Stress Scales (DASS-21) to assess an individual’s mental and psychological health by measuring emotional distress in three sub-categories: depression, anxiety, and stress. This part contained 21 items, which were rated based on the “over the past week” experience of the individual by using a four-point rating scale (0 = “Did not apply to me at all” to 3 = “Applied to me very much, or most of the time”) [18]. The full questionnaire has been validated for use in Malaysia before in other studies [17,19,20]. The average time required for the participants to answer the questionnaire was around 10 to 15 minutes.
Statistical Analysis
Statistical analysis was conducted using IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, N.Y., USA). Descriptive statistics were used to summarize the socio-demographic characteristics of the respondents. Based on their normal distribution, the numerical data were presented as mean, median, and standard deviation. Categorical data were presented as frequency and percentage. Parametric and non-parametric tests based on the normal distribution of data were used to investigate differences between groups. Pearson Chi-square test was used to determine the association between two or more proportions. Mann-Whitney U and Kruskal-Wallis tests were used to determine differences between two or more groups. A partial correlation analysis was done to determine the correlation between two continuous variables. Meanwhile, simple and multiple linear regression were used to identify the relationship between the independent variables (socio-demographic characteristics, depression, anxiety, and stress scores) and the dependent variables (PSQI and MES score). The statistical significance was set at a confidence level of 95%, and a p-value < 0.05.
Ethical Consideration
Ethical approval was obtained from the Human Research Ethics Committee of Universiti Sains Malaysia (Approval No. USM/JEPeM/20040184). Written informed consent was obtained from the study participants.
RESULTS
Demographic Data
The demographic details are presented in Table 1. Most respondents were female (58.8%), Chinese (58.6%), Malay (31.0%), and Indian (4.7%). The other ethnicities were combinations of multi-racial Sabah and Sarawak native minorities, with 5.5%. A greater percentage of responses originated from first-class degree holders (68.5%).
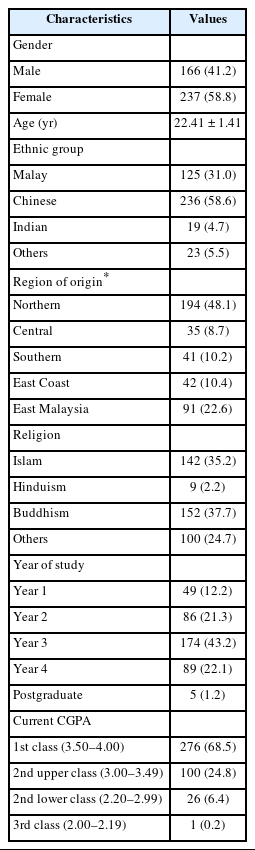
Demographic data (n = 403)
There was no significant association between demographic characteristics and PSQI score (p > 0.05) (Table 2). Besides that, poor-quality sleepers showed a higher percentage (73.7%) than those with good-quality sleep (26.3%). Meanwhile, in terms of age, there was no significant mean difference in good or poorquality sleep (p = 0.831).

Cross-tabulation between poor and good quality sleeper and demographic characteristics (n = 403)
Table 3 shows the relationship between PSQI score and demographics. R2 showed only 7.9% of the variation in the PSQI score could be explained by all the demographic factors (i.e., gender, age, region, and CGPA). In addition, the coefficient for CGPA was 1.04, with a 95% confidence interval (0.64, 1.45) that did not include 0. This indicated a positive and significant relationship between the CGPA and PSQI scores. The t statistic for CGPA (5.055) was much greater than the critical value, and the p-value was less than 0.001, proving that CGPA was a significant predictor of PSQI score. Overall, this linear regression model suggested that CGPA was a significant predictor of PSQI score, while gender, age, and region were not significant predictors.

Relationship between demographic characteristics and PSQI score
The results indicated a significant positive relationship between the PSQI score and the depression score (B = 0.09, 95% CI [0.01, 0.17]), with a t-statistic of 2.15 and a p-value of 0.032. This means that for every one-unit increase in the depression score, the PSQI score was expected to increase by 0.09 units on average. The 95% confidence interval of the coefficient predicts that this effect will most likely range between 0.01 and 0.17 units. Similarly, a significant positive relationship exists between PSQI score and anxiety score (B = 0.13, 95% CI [0.05, 0.22]), with a t-statistic of 0.98 and a p-value of 0.003. This indicated that the PSQI score was expected to increase by an average of 0.13 units for every unit increase in anxiety score. The coefficient’s 95% confidence interval indicated that this effect will likely be between 0.05 and 0.22 units. However, the relationship between PSQI score and stress score was not statistically significant (B = 0.07, 95% CI [-0.02, 0.17]), with a t-statistic of 1.53 and a p-value of 0.128. This indicated that there was no evidence of a significant linear relationship between stress score and PSQI score. The coefficient of determination (R2) for the model was 0.200, which indicated that about 20% of the variation in PSQI scores could be explained by the independent variables (depression, anxiety, and stress scores) in the model (Table 4).
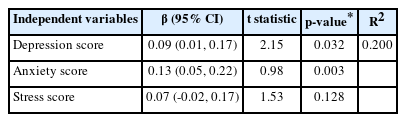
Relationship of PSQI score and depression, anxiety and stress scores category
In Table 5, the R2 has shown that the depression score can explain only 6.2% of the variation in the MES score, anxiety score and stress score. For depression score, the beta coefficient was -0.43, which indicated that as the depression score increased by one unit, the MES score decreased by 0.43 units. This relationship is statistically significant (p < 0.001) with a t statistic of -4.11. For the anxiety score, the beta coefficient is 0.40, which indicated that as the anxiety score increased by one unit, the MES score increased by 0.40 units. This relationship was also statistically significant (p < 0.001) with a t statistic of 3.61. For the stress score, the beta coefficient is -0.05, which indicates that as the stress score increases by one unit, the MES score decreased by 0.05 units. However, this relationship was not statistically significant (p = 0.658) with a t statistic of -0.44. This showed no meaningful relationship exists between the stress score and the MES score. In summary, these results suggested that both the depression score and the anxiety score were related to the MES score, but the stress score was not. The depression score had a negative relationship with the MES score, while the anxiety score had a positive relationship.

Relationship between MES score and depression score, anxiety score and stress score
DISCUSSION
Our study demonstrated that sociodemographic characteristics such as age, gender, year of study, region and CGPA did not significantly affect sleep quality among university students. Similar to the study done by Nurismadiana and Lee [5], 2018 which reported no relationship between sleep quality with gender and CGPA. Surprisingly, respondents with 1st class results had a higher percentage of poor sleep quality than those with better sleep quality, even though the result indicated a non-significant outcome. Another study also showed that academic performance was not significantly related to sleep quality [17]. Again, this result is supported by Nurismadiana and Lee [5], 2018 and Ahmed et al. [21], 2009 where the respondents with good academic performance showed low sleep quality. Both studies did not show any significant association; the current study also indicated a similar outcome. The studies also revealed a significant association between sleep quality and academic stressors, contradicting our outcome [5,21]. Regarding the relationship between age and sleep quality, the present study was in line with a study conducted among undergraduate students in a Nigerian university [4], whereby age was not statistically associated with sleep quality. Nevertheless, a local study disclosed a statistically significant difference between age and quality of sleep [5]. This could be due to younger adults having sleep problems and longer latency [22]. Sanchez et al. [3] found that the higher percentage of female respondents reported poor sleep quality compared to male respondents. This is supported by Nurismadiana and Lee [5], 2018 and the current study, where female respondents had poorer sleep quality than male respondents. Fatima et al. [23] postulated young female adults’ tendency for poor sleep quality is probably caused by gender-based differences in the biology of sleep. However, Lai and Say [17] reported no association between gender and sleep quality, in which the number of good sleepers is the same for both genders. In addition, no significant association was found between gender and sleep quality among undergraduate students in Kuala Lumpur [6]. In contrast with the current study, where years of study did not affect sleep quality, second- and third-year Ethiopian students have significantly higher odds of poor sleep quality [2]. Besides, the year of study was significantly associated with poor sleep quality in a study conducted in Nigeria, where fourth-year seniors reported better sleep quality, implying that students in later years have better coping strategies [4]. However, it is still too general of a statement, as the variations across studies might be due to the differences in social and academic demands across universities [2].
It is well established that sleep quality tends to decline with increasing age [24]. Research has shown that older adults experience more fragmented sleep, more awakenings during the night, and more difficulty falling asleep than younger adults [25]. This decline in sleep quality has been attributed to various factors, including circadian rhythms, hormonal changes, and the increased prevalence of medical conditions [26]. In young adults, insomnia is less common and sleep quality is generally good. This is because younger individuals tend to have more regular sleep patterns and fewer medical conditions that can disrupt sleep. In terms of gender differences, studies have found that women tend to report poorer sleep quality than men, particularly during times of hormonal changes such as pregnancy, menopause, and menstruation [27]. Women are also more likely to experience insomnia and sleep disorders such as restless leg syndrome and sleep apnea [28].
In the current study, among other demographic variables, only CGPA was a significant predictor of PSQI score. A study conducted in Ethiopia elaborated that “good sleepers” university students are more likely to obtain higher mean CGPA than poor sleepers [29]. This finding coincided with another study which supported their hypothesis that poor sleep quality was linked to lower academic performance for nondepressed undergraduate students when a significant negative correlation was observed between Global Sleep Quality (GSQ) score and grade point average (GPA) [30]. Unanticipatedly, a local study reported that PSQI is not correlated with GPA or CGPA; instead, Siah et al. [31] proposed that grit personality may mediate the relationship between sleep quality and CGPA. Grit is a noncognitive trait characterized by perseverance and passion for long-term goals [32]. Academic performance is influenced by various factors, including sleep quality [33]. However, the relationship between sleep quality and academic performance is complex and can be influenced by other factors such as motivation, stress, and mental health [33]. While the effect of age and gender on sleep quality is well established, it is important to consider the complexity of the relationship between sleep quality and academic performance. Other factors, such as motivation and mental health, can also play a significant role in academic performance. Therefore, addressing these factors along with sleep quality may be necessary to improve academic performance in students.
Our study found depression and anxiety as significant predictors of PSQI score, comparable with a previous study [5]. A study done in Nigeria by Seun-Fadipe and Mosaku [4] revealed that respondents with depression, anxiety, and psychological distress had significantly poorer quality of sleep which was consistent with our result, except for psychological distress factors [5]. Similarly, our study is in accordance with another study conducted in Egypt, whereby significant and positive correlations were found between poor sleep quality with depression, anxiety, and stress [34]. Meanwhile, a longitudinal observational study in China suggested a bidirectional relationship between poor sleep quality and depression, anxiety, and stress scores [35].
In the current study, depression and anxiety scores showed a significant linear and positive relationship with the MES scores. In other words, being morning-oriented was associated with depression and anxiety. A similar scenario is observed in a study conducted among Chinese university students, in which students with greater “morningness” reported more depressive symptoms, which the same study assumed was due to the age of the participants (young adults) [36]. Night owls are associated with higher self-reported emotional intelligence (EI) [37], and high EI is related to better mood regulation [38]. In contrast, a study conducted using a different depression scale than our study summarized significant but negative correlation between MES and scores of the three depression scales, which proposed greater “eveningness” could be a triggering factor to become depressed [39]. Contrary to the findings of the current investigation, chronotype is also strongly connected with anxiety in a way that “eveningness” predicted increased anxiety in addition to the effect of sleep disruption [40].
One of the limitations of the present study includes the cross-sectional study design, which impeded the representation of the causal inferences about the association among the covariates and outcome variables within a time frame. Furthermore, almost half of the students in the selected sample were from the northern region of Malaysia, impacting the generalization of the research data since it might over-represent a certain region of Malaysia only. Moreover, the data of the study was obtained from self-reporting by the participants, which is prone to recall bias among the respondents, affecting the reliability of the data.
Conclusion
Poor sleep quality was highly prevalent among university students in Malaysia and was significantly associated with mental health measures. Therefore, improving sleep quality can be an effective strategy for improving mood disorders. Possible interventions include healthy sleep habits, sleep hygiene education, cognitive-behavioral therapy, and pharmacological treatment to enhance sleep quality in individuals with mental health problems. Moreover, early screening and monitoring programs can help identify individuals at high risk of developing mental health issues due to poor sleep quality so that they can receive targeted interventions and support. They can provide resources like access to sleep clinics and peer support groups, implement policies to reduce sleep disruptions during exam periods, and monitor high-risk students using early screening and monitoring programs. The institutions can also encourage a culture of self-care, providing stress-reduction activities such as mindfulness, meditation, and yoga to prioritize students’ well-being.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Authors’ Contribution
Conceptualization: Siew Chin Ong. Data curation: Nizuwan Azman. Formal analysis: Nizuwan Azman. Investigation: Siew Chin Ong. Methodology: Siew Chin Ong. Project administration: Hui Ting Ho. Resources: Siew Chin Ong. Software: Nizuwan Azman. Supervision: Siew Chin Ong. Validation: all authors. Visualization: Hui Ting Ho, Nizuwan Azman. Writing—original draft: all authors. Writing—review & editing: Siew Chin Ong.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Funding Statement
None.