Excessive Daytime Sleepiness and Associated Factors Among Women in Perinatal Period
Article information

Abstract
Background and Objective
Excessive daytime sleepiness (EDS) is an important public health issue requiring adequate screening and management to avoid such harmful consequences. The study aimed to assess the prevalence and risk factors of EDS in the perinatal period.
Methods
Institution-based cross-sectional study was carried out in selected public health institutions of Ethiopia on systematic selected 362 women during perinatal period. We used a validated Epworth daytime sleepiness tool to collect data. Epi-InfoTM 7 and SPSS version 26 were used for data entry and analysis, respectively. Bivariable and multivariable binary logistic regression analyses were conducted to determine the associated factors.
Results
The prevalence of EDS was 16.6% (95% CI: 12.6–20.7). Excessive pregnancy-related concern (adjusted odds ratio [AOR] = 0.232, 95% CI: 0.087–0.621), having depression symptoms (AOR = 8.045, 95% CI: 3.375–19.174), anxiety symptoms (AOR = 4.905, 95% CI: 2.083– 11.550) and having a chronic medical illness (AOR = 5.441, 95% CI: 2.273–13.021) were the factors associated with EDS.
Conclusions
The results of the current study suggested that perinatal EDS among women in northern part of Ethiopia is a highly prevalent and associated with excessive pregnancy concern, depression, anxiety, and medical illness.
INTRODUCTION
The perinatal period is a time characterized by several physical and emotional changes. During the perinatal period several structural, hormonal and other body chemicals were changed [1], as a result, women were highly vulnerable to emotional and psychological conditions such as sleep disturbance, mood, anxiety and others that influence the mother and child’s development and health [2,3]. It is also characterized by a decrease in physical structure and strength, a feeling of fatigue, breastfeeding, and role transition, which results in a painful effect on the mothers and their child’s health [2-4].
Sleep is a natural, temporal state of mind, in which an individual becomes physically inactive, has lower body function and is unaware of the surrounding environment [1,5]. Physical, psychological, social and hormonal changes during the perinatal period disturb women’s sleep patterns [4,6,7]. Sleep problems in the perinatal period, especially during pregnancy, are common health problems [6,7]. A recent study showed that 76%–97% and 33.2% of women experienced sleep problems in the antenatal and postnatal periods, respectively [3].
The common form of sleep disorder during the perinatal period is hyper somnolence (waking up in the middle of the night, daytime sleepiness, and sleeplessness) or insomnia, sleep-related movement disorders, and sleep-related breathing disorders [8-10]. Excessive daytime sleepiness (EDS) is a common public health concern and is a direct and/or indirect predictor for other sleep-related and non-sleep-related problems. It is also characterized by difficulty staying awake and alert during the major waking episodes of the day [4,7].
EDS is one of the most frequent sleep complaints in various populations [11,12], and highly associated with disability [11], and also leads to a deleterious impact on health [13,14]. EDS plays a major role in influencing the mental and physiological health status of women [3,4,7]. The prevalence of EDS among different study populations was 49% in the USA [15], 11% in Canada [16], 13.2% in Korea [17], 18.9% in Japan [11], 33% in France [18], 13.6% in Australia [19], and 31.07% in Ethiopia [13].
Various study revealed that younger age [20-23], high school educational level [24] unemployment status [25], respiratory comorbidity [16], having depression symptoms [21,23,26-29], low body mass index, high degree of workload [22], the presence chronic medical illness such as diabetes mellitus [24,30], being pregnant [25], use of selective serotonin reuptake inhibitors [23], having anxiety symptoms and substance use like smoking [28] were factors associated with EDS.
Sleepiness affects performance differently. It is linked to sleepy periods happening while performing tasks that need a lot of concentration, such driving a car, and may create obvious disturbances in social or occupational functioning [19]. Sleepiness also causes a broad range of neuropsychological deficits, including cognitive dysfunction, depression, and irritability [13,19,20,31]. Additionally, this degree of impairment in women during perinatal time may result in clear wakefulness, morbidity, accidents on herself and their child, and a variety of job and social situation limitations [32].
Permanent EDS can cause deprived health status [11], poor quality of life [16], increased risk of accidents [11], limit productivity and social connections [33], psychological or mental distress [4,7], and poor academic performance. In Ethiopia, there is a scarcity of studies concerning EDS among women and no study was conducted among women in the perinatal period. So, the current study intended to determine the magnitude of perinatal EDS and identify associated factors among women in Ethiopia.
METHODS
Participants
A total of 362 women was determined using a single population proportion formula with the following assumptions; the magnitude of EDS (prevalence = 31.07% [13]), 95% confidence interval (CI), the margin of error (d) = 5% and adding 10% nonresponse rate. The researcher recruited the study respondents using a systematic random sampling method for a period spanning from March, 1, 2022, to June, 15, 2022. Since the total number of women that get a perinatal service per month was 1430 and the number of required test subjects was 362, a sampling interval of four was used as the constant difference between subjects. The first starting number of each study site was picked randomly using the lottery method from the registration counter. Inclusion criteria for the enrolling women were age of ≥ 18 years, having regular antenatal care and postnatal care follow-up, as well as women who would come for delivery during the study period if they were volunteers. Women who are unable to hear or speak and the severely ill who did not fully complete the questionnaires were excluded from the study.
Study Design and Data Collection
A cross-sectional study was carried out with a structured interviewer-administered questionnaire to obtain socio-demographic information including residence, age, educational level, occupation, chronic diseases, including hypertension, diabetes, tuberculosis, and other relevant associated information, from the respondents. Through data collection and processing, complete confidentiality was obtained from unnamed questionnaires. Before starting the questionnaire, written consent was obtained from every participant.
Perinatal EDS was assessed by using the Amharic (a regional language that is widely understood in the society) translated version of the Epworth daytime sleepiness scale, which was validated in Ethiopia [32] with a reliability test of 0.725, which is acceptable [13] and contains eight situations commonly encountered in daily life. The total score of the ESS ranged from 0 to 24. The higher the score, the greater the possibility the individual will fall asleep during the daytime [11,14,25,27,30,33,34]. All women were classified according to ESS score. Those women who scored > 10 were included in the sleepy group and those women who scored ≤ 10 were included in the non-sleepy group [11,14,24,25,27,29,30,33-37].
Depression, anxiety, and stress were assessed using the Depression, Anxiety, and Stress Scale-21 (DASS-21). DASS-21 was a valid, reliable and a wide dimensional measure of psychological distress [38,39]. It has been widely used in studying perinatal psychological health [38-42]. Each item in DASS-21 was rated using a 4-point scale (0 for always false or not applicable to 3 for always true or totally applicable). DASS-21 is a validated tool in Ethiopia with the internal consistency reliability of Cronbach’s alpha of 0.75, 0.72, 0.86, and 0.95 for depression, anxiety, stress, and total scales, respectively [43]. Higher scores indicated greater distress levels. The cut-off values for DASS depression, anxiety and stress were 9, 7, and 14, respectively [38,41]. Based on the will of the women, those who had scores for Depression, Anxiety, and Stress Scales higher than the cut point were linked to the psychiatric ward for further diagnostic investigation.
Social support was assessed by the Oslo-3 social support scale, which is a 3-item questionnaire commonly used to assess social support with an internal consistency of α = 0.640 [44]. The scale asked about the ease of getting help from neighbors, the number of people the subjects can count on when there are serious problems, and the level of concern people show for what the subject was doing. A sum-index was obtained by adding the raw scores of the three items. The range was 3–14. The scores were interpreted as; 3–8 (poor social support), 9–11 (moderate social support), and 12–14 (strong social support) [45,46]. For screening of substance use, a modified form of Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST), developed by the World Health Organization (WHO), an international group of substance abuse researchers, was used to detect and manage substance use and related problems in primary and general medical care settings.
Obstetric variables, such as pregnancy and labor complications, previous histories of stillbirth and previous history of abortion, planned current pregnancy, current pregnancy complications, and previous psychiatric histories, were collected by a structured and pre-tested questionnaire. A structured questionnaire was also used to collect information about the baby’s father’s support, the partner’s feelings about the current pregnancy, and substance use history.
Four Bachelor of Science graduating female clinical nurses and two Master of Science-graduating public health professionals were recruited as data collectors and supervisors, respectively. We modified the standard questionnaire for the evaluation of EDS and other parameters in order to attain data quality. A one-day training was given to both groups on the basic techniques of data collection procedures. One week before the actual data collection, a pretest was performed on 10% of the sample size in Haroye Health Post, and the data was not included in the final study. Daily supervision of the data collection process was implemented. The completeness and consistency of the collected data were checked daily by the supervisors and the principal investigator. The ethical approval of the study was received by the Institutional Review Board (IRB) of Wollo University College of Medicine and Health Science, Ethiopia (approval number: RCSPG-191/14). Ethical permission was obtained from Kutaber district Health office and Boru Meda Hospital. Before starting to fill out the questionnaire, written consent was obtained from every participant.
Statistical Analysis
Data entry was performed using Epi-InfoTM version 7.1 (CDC, Atlanta, GA, USA). After full inspection of its completeness and consistency, it was then exported into Statistical Package for the Social Sciences SPSS window version 26 (IBM Corp., Armonk, NY, USA), for analysis. Categorical descriptive results were expressed using an actual number (frequency). To determine the association between independent and dependent variables, binary logistic regression was performed. Variables in bivariable analysis with a p < 0.2 were selected for multivariable logistic regression. In multivariable analysis, variables with a p < 0.05 with a 95% CI were considered significant factors of EDS. Hosmer and Lemshow goodness of fit tests were performed to assess model fitness at p > 0.05. Besides p-values, crude odds ratio and adjusted odds ratio (AOR) with 95% CI were reported.
RESULTS
In this study a total of 362 participants were included. The mean age of the participants was 30.4 ± 5.47 years. The minimum and maximum age of study subject were 18 and 45 years, respectively. Of these, 240 (66.3%) were found in 24–35 age group, 225 (62.2%) were rural residents. Most of the participants were Amhara in ethnicity (345, 95.3%), and were married (283, 78.2%), and 192 (53.0%) had housewife employment status (Table 1).
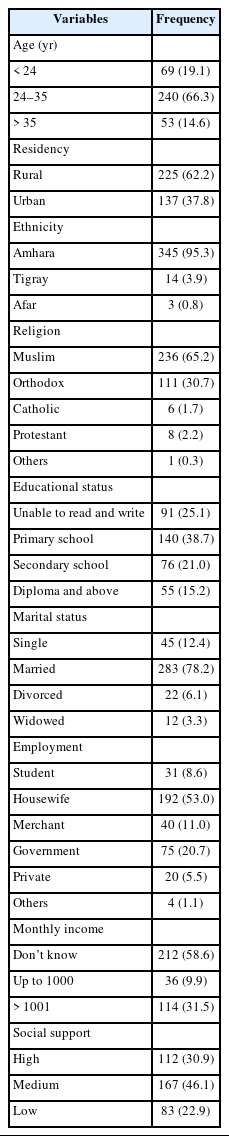
Sociodemographic characteristics of study subjects (n = 362)
On pregnancy-related factors, 284 (78.5%) had a happy feeling of being pregnant; 267 (73.8%) reported that pregnancy was planned; 143 (39.5%) experienced excessive pregnancy-related feelings, 270 (74.6%) were delivered through normal vaginal delivery; and 171 (47.2%) had a history of obstetric complication.
Clinically, 147 (40.7%) people used substances in the past three months, 107 (29.6%) had a DASS-21 ≥ 10 of depression scale, and 90 (24.9%) had a chronic medical illness (Table 2).
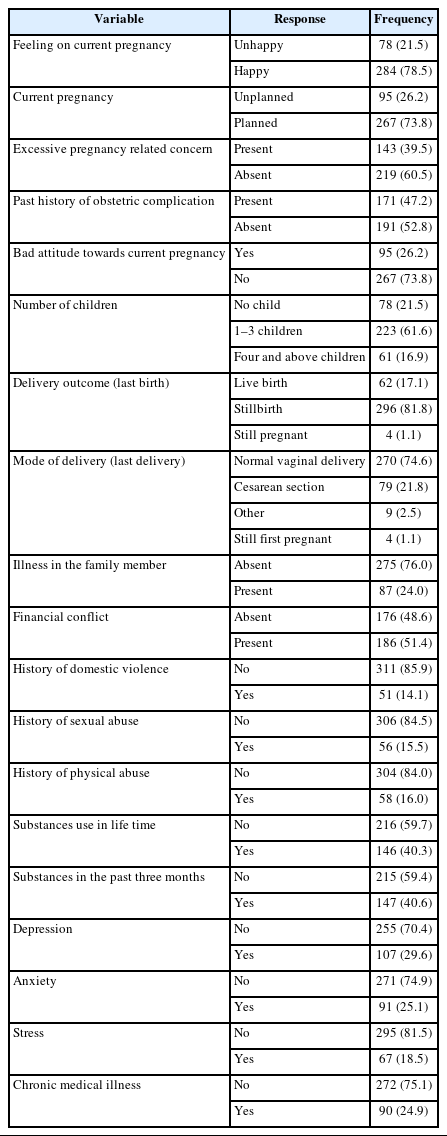
Pregnancy and clinical characteristic of study subject (n = 362)
Epworth Sleep Scale Scores of Respondents
The lowest score of the data was 0 and the highest score was 19. The mean, median and mode the respondent was 6.8 ± 3.74, 7, 6, respectively. The scores above 10 were considered as the presence of excessive day time sleepiness (Fig. 1).
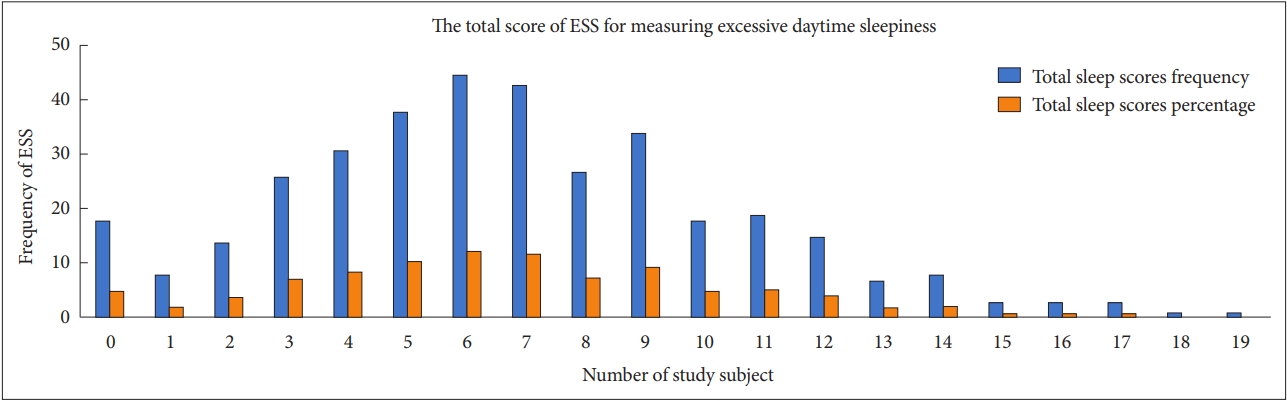
The frequency of the Epworth Daytime Sleepiness Scale (ESS) response among women in perinatal period (n = 362).
Accordingly, out of the 362 study subjects recruited for the study, 60 (16.6%) fulfilled the criteria for EDS as measured by the ESS. EDS (ESS score ≥ 11) was noted in 60 (16.6%) participants (Fig. 2).
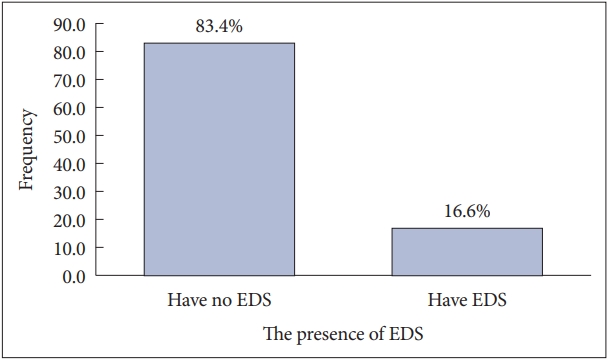
The prevalence of excessive daytime sleepiness (EDS) among women in perinatal period (n = 362).
Factors Associated with EDS
After controlling for confounding effect of variables, excessive pregnancy related concern (AOR = 0.232, 95% CI: 0.087–0.621), having depression symptoms (AOR = 8.045, 95% CI: 3.375–19.174), anxiety symptoms (AOR = 4.905, 95% CI: 2.083–11.550) and having chronic medical illness (AOR = 5.441, 95% CI: 2.273–13.021) were the determinant factor of EDS (Table 3).

Factors associated with excessive daytime sleepiness in perinatal period (n = 362)
DISCUSSION
Sleepiness affect performance in different ways. It is associated with sleepy episodes occurring during activities requiring a high degree of attention (driving a car) and may cause noticeable disruptions in social or occupational functioning [19]. Sleepiness also causing a broad range of neuropsychological deficits, including cognitive dysfunction, depression, and irritability [13,19,20,47]. Additionally, this degree of impairment in women during perinatal time may result in clear wakefulness, morbidity, accidents on herself and their child, and a variety of job and social situation limitations [48].
The aim of this study was to assess the prevalence of EDS and associated factors among women in the perinatal period at Kutaber Health Facility and Boru Meda General Hospital. The overall prevalence of EDS was 16.6% (95% CI: 12.6–20.7).
This result is in line with the other study conducted in Australia 13.6% [19] and 12.6% [49], in France 18.9 [50], in United Kingdom 18% [51], in Japan 14.9% [36] and 18.9% [29], in Korea 13.2% [17]. The finding in this study was higher when compared with the other study conducted in Switzerland 5.1% [31], in Japan 2.5% [52], in Slovakia 10.2% [30], in Sweden 7.9% [28], in China 10.9% [53]. In contrast, this result was less than the other study conducted in France 28% [18], in Korea 19.1% [47], in Brazil 55.5% [21], in France 35.3% [22], in Belgium 50.8% [33] and 34.3% [27], in China 22.2% [24], in Greece 38.8% [54] and in Nigeria 44.8% [55]. The discrepancy might be a result of a difference in assessment tools, geographical areas, sample size, the nature and culture of the study subject, and the study setting.
On the determinant factor, women with excessive pregnancy-related concern (AOR = 0.232, 95% CI: 0.087–0.621) experienced more daytime sleepiness than those who did not have excessive concern. This was due to excessive concern, which disturbs the internal function of the body system and leads to different complications like increased blood pressure, depression, anxiety, and others. Such type of complication especially depression leads daytime sleepiness.
The odds of having depression symptoms in perinatal time (AOR = 8.045, 95% CI: 3.375–19.174) were 8 times higher than those who have not depression symptoms. The result was analogous to other studies conducted in France [18], Brazil [21], two different studies in Australia [19,49], and New Zealand [56], and in Korea [47]. This might be because higher levels of cortisol, corticotropic releasing hormone, and norepinephrine during depression lead to sleep rhythm disruption that ends up with EDS [55]. Sleeping too much could be a symptom of depression.
Parallel to many other studies conducted elsewhere [15,52], the odds of having anxiety symptoms (AOR = 4.905, 95% CI: 2.083–11.550) were four times higher than those who did not show anxiety symptoms. These may be due to long-term exposure to anxiety, which causes the hypothalamus, pituitary, and adrenal glands to release hormones to prepare for fight, flee, or freeze. In response they experienced a feeling of exhaustion, were physically fatigued, and may have difficulty falling asleep or staying asleep at night. Otherwise, they may oversleep during the day.
The odds of having chronic medical illness (AOR = 5.441, 95% CI: 2.273–13.021) were five times greater than for those women without chronic medical illness. This was consistent with other study in France [50] and [18], Canada [16], Australia [19] and Slovakia [30]. The possible clarification is the pain and fatigue of chronic medical illness have impact on women daily activities including sleep quality [16,19,50]. Because of their illness they often experience sleeping problems at night and they become sleepy during day time. Indirectly, the illness also leads other health problems like depression and/or anxiety, which can also cause EDS.
Other study also reported that the association of EDS to younger age [20,52] male sex [49,52], smoking [18], high degree of job [22], insomnia [13,18], loud snoring [16,20,52], and multiple gestations [20]. Though, all the above factors were not independent predictors of EDS in our study, this might be due to variations in sample size, life style, health status, and sociocultural factors of the study subjects. The findings of this study suggested that women in perinatal period are susceptible to EDS that is associated with depression, anxiety and medical illness. If not appropriately handled, EDS could lead to poor quality of maternal and child health [48]. Objective measures of sleepiness were not available for this study. So, the study has some limitations. Selection bias may exist even if systematic random selection was used for the recruitment of the participants. The responses the questionnaire may depend on the participant’s perceptual experience as a result recall bias occurred.
In conclusion, perinatal EDS is high and significantly associated with excessive pregnancy-related concern, depression, anxiety, and chronic medical illness. This suggested the need to encourage women to get counseling on how to cope with the pregnancy-related biological, physical, social, and emotional changes in the environment, which is important to reduce the associated factor. Health institutions should establish guidance and counseling services when the women get them during perinatal care. Furthermore, we recommend future researchers undertake studies using strong designs and qualitative studies to find out the factors affecting EDS.
Notes
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
Authors’ Contribution
Conceptualization: Jemal Seid, Emam Mohammed. Data curation: Jemal Seid. Formal analysis: Jemal Seid. Funding acquisition: Emam Mohammed. Methodology: all authors. Project administration: Jemal Seid, Emam Mohammed, Hassen Yimer Hassen. Resources: Jemal Seid, Emam Mohammed. Software: Jemal Seid, Emam Mohammed. Supervision: Jemal Seid, Emam Mohammed, Hassen Yimer Hassen. Validation: Jemal Seid, Bilal Mohammed Aman, Hassen Yimer Hassen. Visualization: all authors. Writing—original draft: Jemal Seid. Writing—review & editing: all authors.
Conflicts of Interest
The authors have no potential conflicts of interest to disclose.
Funding Statement
Kutaber district administrative office provided some funds contribution for data collection procedures.
Acknowledgements
The authors would like to acknowledge the staff of Wollo University, study participants, and data collectors for their welcome and assistance and also to Kutaber district administrative office for allowing funds to conduct this study. Finally, our special gratitude goes to all peoples who formally or informally gave us support to accomplish this study.