Are You Asking What Time Did Your Patients Go to Bed?: Getting the Short Sleep Onset Latency
Article information

Abstract
A few patients diagnosed with insomnia attempt going to bed earlier to obtain adequate sleep and fall asleep less than 30 min, although they often complain about their inability to fall asleep easily. The aim of this study was to explore the association between short sleep latency and patients’ sleepwake pattern. All the 99 patients with primary insomnia who were under treatment with benzodiazepine or non-benzodiazepine gamma-aminobutyric acid (GABA) agonists as sleeping pills were selected. The time to take hypnotics, bedtime, sleep onset, and wake-up times were determined from medical records. Subjects who showed sleep latency of less than 30 min (SL ≤ 30, n = 56) were treated with hypnotics (10:46 pm) before going to bed (11:00 pm) later compared with subjects with sleep latency greater than 30 min (SL > 30 min, n = 43, hypnotic ingestion time, 9:46 pm; bedtime 10:10 pm). Duration from wake-up time to bedtime (WTB) was significantly longer in SL ≤ 30 group (16.5 ± 1.1 h) compared to SL > 30 group (15.8 ± 1.5 h). Long sleep latency was significantly correlated with old age, earlier ingestion of sleeping pills, earlier bedtime, and short duration of WTB (all, p < 0.01). Early bed time in the evening was not associated with short sleep latency. Patients with insomnia may find that delayed bedtime may promote faster sleep.
INTRODUCTION
Insomnia is one of most frequent and disturbing symptoms. When patients cannot easily fall asleep, they tend to worry about the consequences of insomnia. Based on a 3P behavioral model of insomnia [1], maladaptive sleep hygiene or dysfunctional thinking acts as a factor perpetuating chronic insomnia. Furthermore, these dysfunctional beliefs about sleep [2] can also influence the severity of insomnia. Patients with dysfunctional beliefs about their insomnia often prefer to go to bed early in the evening to obtain quick sleep [3]. A few patients believe that early bedtime may induce early sleep onset. Especially, elderly patients believe in falling asleep early in the evening [2], and advanced circadian rhythm of sleep-wake cycle was associated with aging [4].
Sleep latency less than 30 min is considered as an indicator and the most defensible quantitative element of good sleep [5]. Patients trying to reduce sleep latency less than 30 min after their bedtime, and normal sleep onset latency were defined as less than 30 min in numerous studies [6,7]. In the clinical trials with hypnotics [8,9] or non-pharmacological treatment for insomnia [10,11], sleep latency less than 30 min was defined as an indicator of effectiveness. In clinical practice, general physicians who were not trained in sleep medicine do not often ask the patients about their sleep structure such as bedtime, sleep onset time, and wake-up time, when they prescribe sleeping pills.
We hypothesized in this study that short sleep latency, sleep onset latency within 30 min (SL ≤ 30 min), is related to their bedtime or sleep onset time. Bedtime or wake-up time is also related to age. The aim of this study was to explore whether short sleep latency was associated with patients’ bedtime and sleep onset time.
METHODS
In this retrospective review and analysis of medical records, participants’ informed consent was not required. The study protocol was approved by the Institutional Review Board of the Asan Medical Center (2018–0406). We collected the information of subjects who were diagnosed with primary insomnia and treated with hypnotics including benzodiazepine or non-benzodiazepine gamma-aminobutyric acid (GABA) agonists during their first visit to the sleep clinic at the Department of Psychiatry in the Asan Medical Center, Seoul, between July 2014 and February 2018. A psychiatrist and a sleep specialist (S.C.) routinely assessed patients’ psychiatric history or sleep disorders and obtained a diagnosis of primary insomnia according to the diagnostic criteria of the International Criteria for Sleep Disorders-2nd edition.
Patients were excluded if they had 1) major psychiatric illnesses such as major depressive disorder or major psychosis; 2) other sleep disorders such as circadian rhythm sleep disorder, restless legs syndrome, or periodic limb movements during sleep; 3) snoring or apnea symptoms suggestive of obstructive sleep apnea syndrome; 4) major medical or neurological diseases, which may limit their daily activities; 5) history of cognitive-behavioral therapy for insomnia; 6) usually spending more than 30 min lying on their bed during daytime; or 7) other treatment with psychotropic medications such as antipsychotics, antidepressants, or melatonin agonists as sleeping pills.
In the clinic, we always ask: 1) “How many tablets of sleeping pills per day are you taking now?” 2) “Are you satisfied with your sleeping pills to induce sleep?” 3) “What is the usual time to take sleeping pills?” 4) “What is your usual bedtime?” 5) “What is your usual time to fall asleep?” 6) “What is your usual time to finally get out of bed in the morning?” [12]. After reviewing subjects’ medical records, we categorized patients into sleep latency of 30 min or less (SL ≤ 30) and sleep onset latency greater than 30 min (SL > 30).
Calculating the Time and Duration Variables
The time and duration variables were calculated by averaging the usual times reported; if a patient answered “I went to bed usually between 9:00 pm and 9:30 pm,” we calculated this time as 9:15 pm. Based on the data, we calculated the time variables including hypnotic administration time, bedtime, sleep onset time, and wake-up time. In addition, based on the time variables, we determined the duration variable including sleep onset latency (SL), time in bed (TIB), duration from pills to bedtime (PTB), duration from pills to sleep onset time (PTS), and duration from pills to wake-up time (PTW) [12], duration from wake-up time to bedtime (WTB), and duration from wakeup time to sleep onset time (WTS).
Calculating the Number of Tablets of Equivalent Hypnotic Drugs
The “number of tablets of equivalent hypnotic drugs (TEQ)” was calculated using an equivalent dosage of each hypnotic consumed by the patient [13]; alprazolam (0.25 mg), bromazepam (3 mg), clonazepam (0.25 mg), diazepam (5 mg), lorazepam (0.5 mg), triazolam (0.25 mg), and zolpidem (10 mg of immediate-release form and 12.5 mg of extended-release form). The TEQ was calculated by summing the number of prescribed tablets of sleeping pills per day.
Statistical Analysis
Statistical analyses were performed with SPSS ver. 21.0 for Windows (IBM Corp., Armonk, NY, USA). The level of significance was defined as p < 0.05 in two-tailed tests for all analyses. A Student’s t-test was conducted for continuous variables and chi-squared test was done for categorical variables. A Pearson correlation analysis was performed to explore the association among variables.
RESULTS
Among 99 subjects in this study, the sleep latencies of 56 (57%) were less than 30 min (SL ≤ 30 group), with a mean age significantly lower compared with the SL > 30 group (Table 1). The mean hypnotic ingestion time was 10:46 pm in the SL ≤ 30 and 9:46 pm in the SL > 30 groups (p < 0.01), and the mean bedtime was 11:00 pm in the SL ≤ 30 group and 10:10 pm in the SL > 30 group (p < 0.01). Sleep onset time was significantly delayed in the SL > 30 group, without any significant difference in wake-up time. Among the duration variables, subjects in both groups followed general verbal instructions of hypnotic dosage around 30 min before bedtime (PTB, 13.2 min vs. 22.8 min, p = 0.053). The duration from pill ingestion to sleep onset (PTS, 34.2 vs. 132.2 min, p < 0.01), the duration from pill ingestion to wakeup time (PTW, 7.7 vs. 8.6 h, p < 0.01), and the duration from wake-up to sleep onset time (WTS, 16.9 h vs. 17.7 h, p < 0.01) were significantly shorter in the SL ≤ 30 group. However, the duration from wake-up to bedtime (WTB, 16.5 h vs. 15.8 h, p < 0.01) was significantly longer in the SL ≤ 30 group compared with SL > 30 group. No significant difference in the TEQ was observed (p = 0.21).
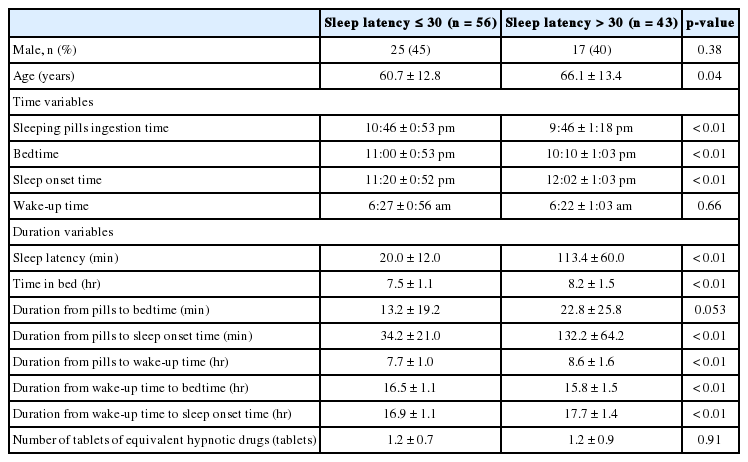
Clinical characteristics of patients with sleep latencies 30 minutes or less
Sleep latency was significantly correlated with age (r = 0.27, p < 0.01). Among the time variables, earlier sleeping pill ingestion time (r = −0.56, p < 0.01) and earlier bedtime (r = −0.54, p < 0.001) was correlated with long sleep latency. Among duration variables, extended time in bed, long PTS, long PTW, and short WTB were significantly correlated with long sleep latency (all, p < 0.01) (Table 2). Old age was associated with early bedtime, long sleep latency, and long PTS and WTS (all, p < 0.05). The high TEQ was correlated with early sleep onset time (p < 0.01), long time in bed, long PTW, short WTB, and short WTS.
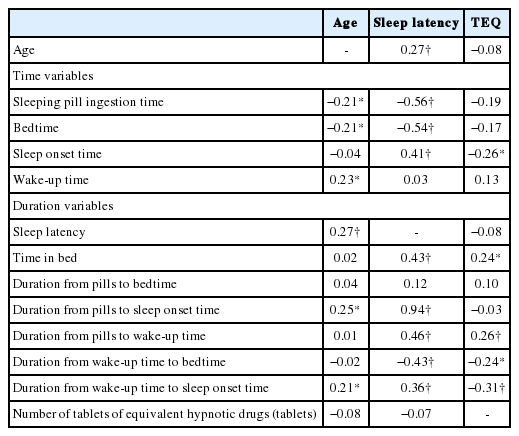
Pearson’s correlation analysis of sleep latency with clinical characteristics of insomnia (n = 99)
DISCUSSION
In this study, short sleep latency was associated with late sleeping pill ingestion time and late bedtime, and prolonged the duration from wake-up time to bedtime. In general, patients expect to fall asleep easily by taking sleeping pills. However, a few patients cannot catch a good sleep despite the high dosage of sleeping pills. In this case, patients usually prefer to increase the dosage of their sleeping pills, and physicians also prescribe sleeping pills increasingly or switch to another medication. Patients usually attempt going to bed early in the evening after taking sleeping pills as early as possible to obtain more sleep. Patients’ belief in obtaining at least 8 h of sleep prompts them to go to bed early [14,15]. However, many patients cannot easily fall asleep despite their strategy. Early intake of sleeping pills and early bedtime were significantly correlated with long sleep latency in this study. The results are contrary to patients’ general expectation. These results suggest that ingestion of sleeping pills and early evening bedtime cannot guarantee short sleep latency for patients with insomnia.
Two process model of sleep regulation [16] explains that both circadian rhythm (process C) and homeostatic drive (process S) are important for good sleep. i.e., circadian rhythm alone is not adequate for sleep regulation, and pressure to sleep (homeostatic drive) is also needed to promote good sleep. Even though patients with insomnia try to go to bed early in the evening, they cannot fall asleep in the absence of adequate circadian timing and pressure to sleep. In this study, short sleep latency was correlated with long duration from wake-up time to bedtime (WTB, 16.5 h in SL ≤ 30 group and 15.8 h in SL > 30 group). Low homeostatic drive (long time in bed, long PTW, and short WTB) and early circadian timing (early sleeping pill ingestion and early bedtime) cannot decrease patients’ sleep latency.
Sleeping pills should be prescribed after ascertaining patients’ sleep structure including bedtime, sleep onset time, and wakeup time. In clinical practice, it is not usual for general physicians to ask patients with insomnia about their bedtime and time to wake up in the morning when they prescribe hypnotics to the patients. Elderly patients prefer to go to bed earlier in the evening [2]. However, early bedtime and spending longer in bed will not result in longer sleep. In this study, old age was significantly associated with early bedtime, short duration from administration pills to bedtime, long sleep latency, and long time in bed. It is well known that aging is related with advanced circadian rhythm sleep-wake cycle [4]. In addition, low activity and reduced work drive them to the bed [17]. However, contrary to the physiological changes associated with aging, elderly patients attempt to sleep too early in the morning. However, good sleep depends on good circadian timing based on a two-process model of sleep regulation [16], and early bedtime cannot guarantee early sleep onset time.
The limitation of this study relates to the lack of analysis of the association between bedtime and short sleep latency in patients with primary insomnia. Late bedtime does not always promote good sleep. Especially, late bedtime is one of the factors leading to reduced sleep duration among children [18] and adolescents [19]. Delayed bedtime may be occasionally associated with sleep disturbances. In this study, we merely tested the hypothesis that early bedtime is not helpful to shorten the sleep latency. Another limitation is the use of sleeping pills in this study. Sleeping pills may influence short sleep latency. However, it seems natural, since many patients consume sleeping pills in clinical practice.
In conclusion, we found that early ingestion sleeping pills and going to bed early in the evening do not reduce sleep latency in patients with primary insomnia contrary to patients’ expectation. In clinical practice, patients may be advised to take sleeping pills and go to bed later in the evening to obtain at least 7 h of sleep.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Authors’ Contribution
Conceptualization: Chung S. Data curation: Chung S, Youn S, Formal analysis: Chung S. Investigation: Chung S, Youn S, Kim C. Methodology: Chung S, Youn S. Project administration: Chung S. Resources: Chung S, Youn S, Kim C. Software: Chung S. Supervision: Chung S. Validation: Chung S, Youn S, Kim C. Writing—original draft: Chung S. Writing—review & editing: Chung S, Youn S, Kim C.